

Is venous blood a more reliable description of acid-base state following simulated hypo- and hyperventilation?
- PMID: 33596977
- PMCID: PMC7888697
- DOI: 10.1186/s13049-021-00848-8
Is venous blood a more reliable description of acid-base state following simulated hypo- and hyperventilation?
Abstract
Background: ABGs are performed in acute conditions as the reference method for assessing the acid-base status of blood. Hyperventilation and breath-holding are common ventilatory changes that occur around the time of sampling, rapidly altering the 'true' status of the blood. This is particularly relevant in emergency medicine patients without permanent arterial catheters, where the pain and anxiety of arterial punctures can cause ventilatory changes. This study aimed to determine whether peripheral venous values could be a more reliable measure of blood gases following acute changes in ventilation.
Methods: To allow for characterisation of ventilatory changes typical of acutely ill patients, but without the confounding influence of perfusion or metabolic disturbances, 30 patients scheduled for elective surgery were studied in a prospective observational study. Following anaesthesia, and before the start of the surgery, ventilator settings were altered to achieve a + 100% or - 60% change in alveolar ventilation ('hyper-' or 'hypoventilation'), changes consistent with the anticipation of a painful arterial puncture commonly encountered in the emergency room. Blood samples were drawn simultaneously from indwelling arterial and peripheral venous catheters at baseline, and at 15, 30, 45, 60, 90 and 120 s following the ventilatory change. Comparisons between the timed arterial (or venous) samples were done using repeated-measures ANOVA, with post-hoc analysis using Bonferroni's correction.
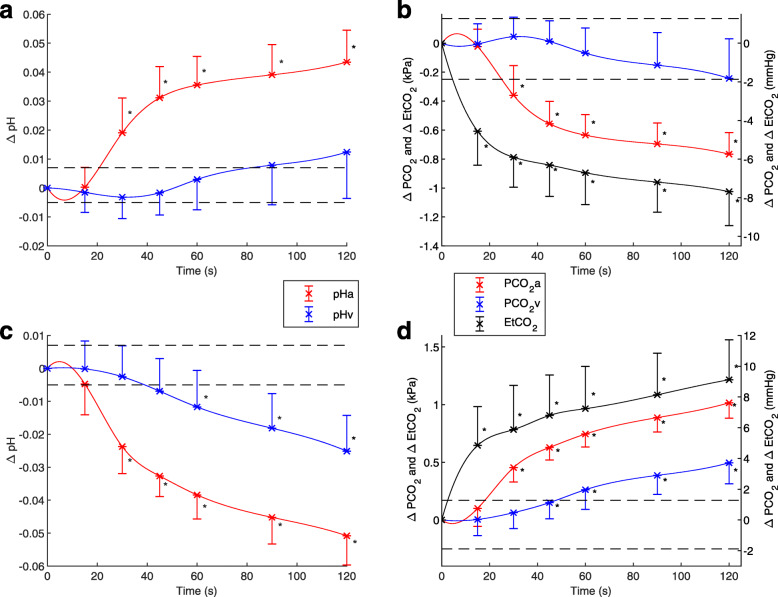
Results: Arterial blood pH and PCO2 changed rapidly within the first 15-30s after both hyper- and hypoventilation, plateauing at around 60s (∆pH = ±0.036 and ∆PCO2 = ±0.64 kPa (4.7 mmHg), respectively), with peripheral venous values remaining relatively constant until 60s, and changing minimally thereafter. Mean arterial changes were significantly different at 30s (P < 0.001) when compared to baseline, in response to both hyper- and hypoventilation.
Conclusion: This study has shown that substantial differences in arterial and peripheral venous acid-base status can be due to acute changes in ventilation, commonly seen in the ER over the 30s necessary to sample arterial blood. If changes are transient, peripheral venous blood may provide a more reliable description of acid-base status.
Keywords: Acid-base; Arterial; Blood gas analysis; Hyperventilation; Hypoventilation; Venous.
Conflict of interest statement
SER and SK were previous shareholders of OBI Medical A/S.
Figures
Similar articles
-
Mathematically arterialised venous blood is a stable representation of patient acid-base status at steady state following acute transient changes in ventilation.J Clin Monit Comput. 2022 Oct;36(5):1333-1340. doi: 10.1007/s10877-021-00764-3. Epub 2021 Oct 13. J Clin Monit Comput. 2022. PMID: 34647198 Free PMC article.
-
Changes in central venous to arterial carbon dioxide gap (PCO2 gap) in response to acute changes in ventilation.BMJ Open Respir Res. 2021 Mar;8(1):e000886. doi: 10.1136/bmjresp-2021-000886. BMJ Open Respir Res. 2021. PMID: 33737311 Free PMC article.
-
Serial observations of arterial and mixed-venous blood gases after step change in ventilation.Pflugers Arch. 1975;353(2):123-38. doi: 10.1007/BF00599873. Pflugers Arch. 1975. PMID: 1167666
-
Comparing Central Venous Blood Gas to Arterial Blood Gas and Determining Its Utility in Critically Ill Patients: Narrative Review.Anesth Analg. 2021 Aug 1;133(2):374-378. doi: 10.1213/ANE.0000000000005501. Anesth Analg. 2021. PMID: 33780397 Review.
-
Review article: Can venous blood gas analysis replace arterial in emergency medical care.Emerg Med Australas. 2010 Dec;22(6):493-8. doi: 10.1111/j.1742-6723.2010.01344.x. Emerg Med Australas. 2010. PMID: 21143397 Review.
Cited by
-
Comparison of mathematically arterialised venous blood gas sampling with arterial, capillary, and venous sampling in adult patients with hypercapnic respiratory failure: a single-centre longitudinal cohort study.BMJ Open Respir Res. 2023 Jun;10(1):e001537. doi: 10.1136/bmjresp-2022-001537. BMJ Open Respir Res. 2023. PMID: 37369550 Free PMC article.
-
Mathematically arterialised venous blood is a stable representation of patient acid-base status at steady state following acute transient changes in ventilation.J Clin Monit Comput. 2022 Oct;36(5):1333-1340. doi: 10.1007/s10877-021-00764-3. Epub 2021 Oct 13. J Clin Monit Comput. 2022. PMID: 34647198 Free PMC article.
-
Carbon Dioxide and Hemoglobin at Presentation with Hypertrophic Pyloric Stenosis-Are They Relevant? Cohort Study and Current Opinions.Children (Basel). 2025 Jul 4;12(7):885. doi: 10.3390/children12070885. Children (Basel). 2025. PMID: 40723078 Free PMC article.
-
Trending peripheral venous PCO2 in patients with respiratory failure using mathematically arterialised venous blood gas samples.BMJ Open Respir Res. 2021 May;8(1):e000896. doi: 10.1136/bmjresp-2021-000896. BMJ Open Respir Res. 2021. PMID: 34049866 Free PMC article.
References
-
- Cakar N, Tu M, Demirarslan A, Nahum A, Adams A, Akyncy O, et al. Time required for partial pressure of arterial oxygen equilibration during mechanical ventilation after a step change in fractional inspired oxygen concentration. Intensive Care Med. 2001;27:655–659. doi: 10.1007/s001340100900. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
