

Feasibility of continuous monitoring of vital signs in surgical patients on a general ward: an observational cohort study
- PMID: 33597138
- PMCID: PMC7893648
- DOI: 10.1136/bmjopen-2020-042735
Feasibility of continuous monitoring of vital signs in surgical patients on a general ward: an observational cohort study
Abstract
Objective: To determine feasibility, in terms of acceptability and system fidelity, of continuous vital signs monitoring in abdominal surgery patients on a general ward.
Design: Observational cohort study.
Setting: Tertiary teaching hospital.
Participants: Postoperative abdominal surgical patients (n=30) and nurses (n=23).
Interventions: Patients were continuously monitored with the SensiumVitals wearable device until discharge in addition to usual care, which is intermittent Modified Early Warning Score measurements. Heart rate, respiratory rate and axillary temperature were monitored every 2 min. Values and trends were visualised and alerts sent to the nurses.
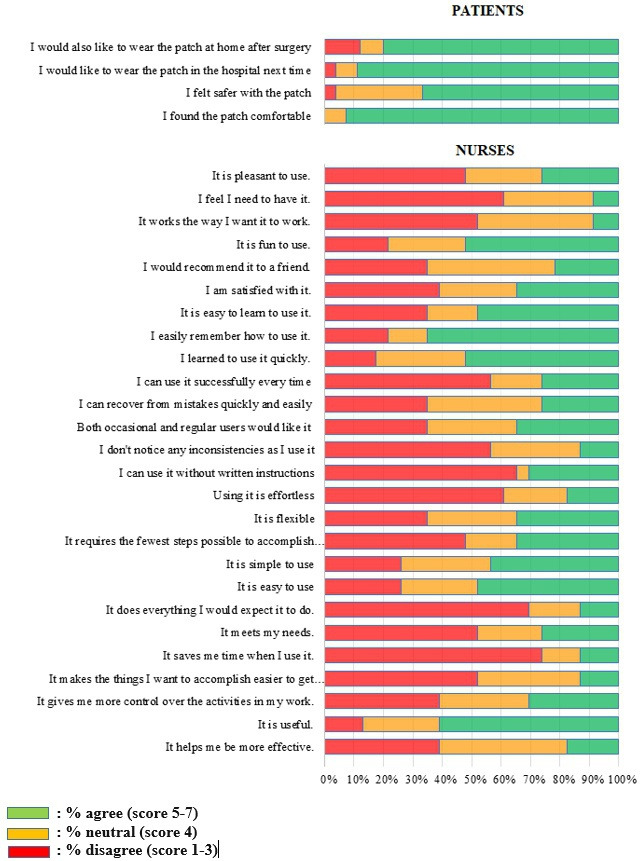
Outcomes: System fidelity was measured by analysis of the monitoring data. Acceptability by patients and nurses was assessed using questionnaires.
Results: Thirty patients were monitored for a median duration of 81 hours (IQR 47-143) per patient, resulting in 115 217 measurements per parameter. In total, 19% (n=21 311) of heart rate, 51% (n=59 184) of respiratory rate and 9% of temperature measurements showed artefacts (n=10 269). The system algorithm sent 972 alerts (median alert rate of 4.5 per patient per day), of which 90.3% (n=878) were system alerts and 9.7% (n=94) were vital sign alerts. 35% (n=33) of vital sign alerts were true positives. 93% (n=25) of patients rated the patch as comfortable, 67% (n=18) felt safer and 89% (n=24) would like to wear it next time in the hospital. Nurses were neutral about usefulness, with a median score of 3.5 (IQR 3.1-4) on a 7-point Likert scale, ease of use 3.7 (IQR 3.2-4.8) and satisfaction 3.7 (IQR 3.2-4.8), but agreed on ease of learning at 5.0 (IQR 4.0-5.8). Neutral scores were mostly related to the perceived limited fidelity of the system.
Conclusions: Continuous monitoring of vital signs with a wearable device was well accepted by patients. Nurses' ratings were highly variable, resulting in on average neutral attitude towards remote monitoring. Our results suggest it is feasible to monitor vital signs continuously on general wards, although acceptability of the device among nurses needs further improvement.
Keywords: adverse events; colorectal surgery; health & safety; hepatobiliary surgery; pancreatic surgery; surgery.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Findlay G, Goodwin A, Protopappa K, et al. Knowing the risk: a review of the peri-operative care of surgical patients. London: National Confidential Enquiry into Patient Outcome and Death, 2011.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical