

Safety and efficacy of hydrothermal duodenal mucosal resurfacing in patients with type 2 diabetes: the randomised, double-blind, sham-controlled, multicentre REVITA-2 feasibility trial
- PMID: 33597157
- PMCID: PMC8761999
- DOI: 10.1136/gutjnl-2020-323608
Safety and efficacy of hydrothermal duodenal mucosal resurfacing in patients with type 2 diabetes: the randomised, double-blind, sham-controlled, multicentre REVITA-2 feasibility trial
Abstract
Objective: Hydrothermal duodenal mucosal resurfacing (DMR) is a safe, outpatient endoscopic procedure. REVITA-2, a double-blind, superiority randomised controlled trial, investigates safety and efficacy of DMR using the single catheter Revita system (Revita DMR (catheter and system)), on glycaemic control and liver fat content in type 2 diabetes (T2D).
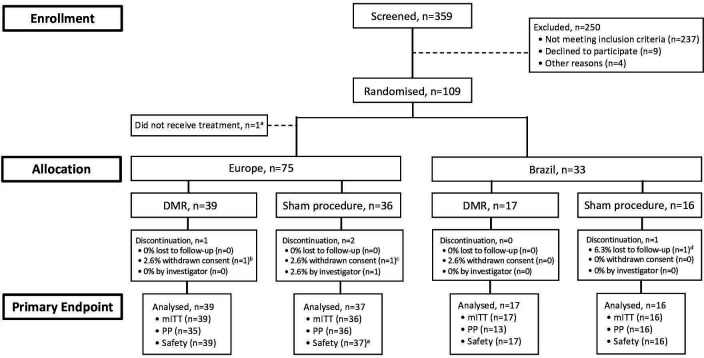
Design: Eligible patients (haemoglobin A1c (HbA1c) 59-86 mmol/mol, body mass index≥24 and ≤40 kg/m2, fasting insulin >48.6 pmol/L, ≥1 oral antidiabetic medication) enrolled in Europe and Brazil. Primary endpoints were safety, change from baseline in HbA1c at 24 weeks, and liver MRI proton-density fat fraction (MRI-PDFF) at 12 weeks.
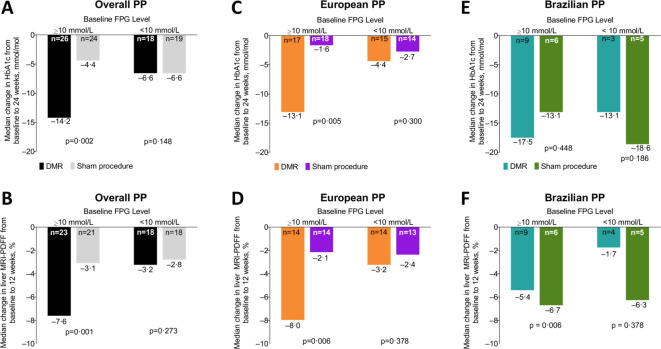
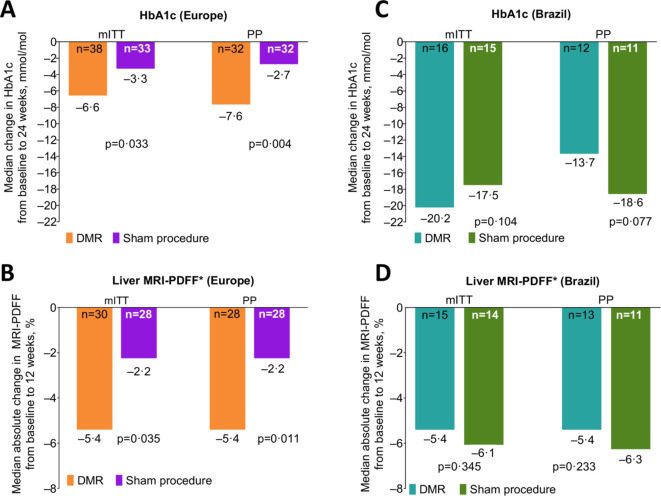
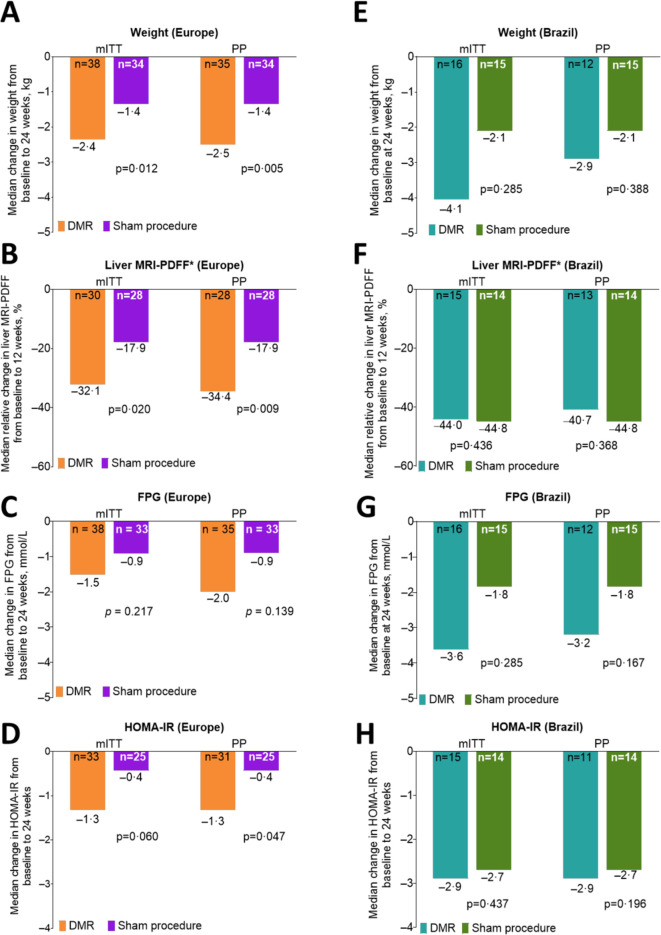
Results: Overall mITT (DMR n=56; sham n=52), 24 weeks post DMR, median (IQR) HbA1c change was -10.4 (18.6) mmol/mol in DMR group versus -7.1 (16.4) mmol/mol in sham group (p=0.147). In patients with baseline liver MRI-PDFF >5% (DMR n=48; sham n=43), 12-week post-DMR liver-fat change was -5.4 (5.6)% in DMR group versus -2.9 (6.2)% in sham group (p=0.096). Results from prespecified interaction testing and clinical parameter assessment showed heterogeneity between European (DMR n=39; sham n=37) and Brazilian (DMR n=17; sham n=16) populations (p=0.063); therefore, results were stratified by region. In European mITT, 24 weeks post DMR, median (IQR) HbA1c change was -6.6 mmol/mol (17.5 mmol/mol) versus -3.3 mmol/mol (10.9 mmol/mol) post-sham (p=0.033); 12-week post-DMR liver-fat change was -5.4% (6.1%) versus -2.2% (4.3%) post-sham (p=0.035). Brazilian mITT results trended towards DMR benefit in HbA1c, but not liver fat, in context of a large sham effect. In overall PP, patients with high baseline fasting plasma glucose ((FPG)≥10 mmol/L) had significantly greater reductions in HbA1c post-DMR versus sham (p=0.002). Most adverse events were mild and transient.
Conclusions: DMR is safe and exerts beneficial disease-modifying metabolic effects in T2D with or without non-alcoholic liver disease, particularly in patients with high FPG.
Trial registration number: NCT02879383.
Keywords: diabetes mellitus; duodenal mucosa; endoscopic procedures; fatty liver.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: GM has received funding/grant support from Novo Nordisk, Fractyl Laboratories, Metacure, Keyron, and honorarium for consultancy from Johnson & Johnson, Novo Nordisk, and Fractyl Laboratories. JD has received research support from Fractyl Laboratories Inc for IRB-approved studies. DH has received honorarium for consultancy and/or speaker fees from Novo Nordisk, Sanofi, Astra Zeneca, Roche, Sunovion, and Fractyl Laboratories. EM has received honorarium for consultancy from Olympus do Brasil and Boston Scientific. CC has received funding/grant support from Novo Nordisk and honorarium for consultancy from Novo Nordisk and Eurofarma. DLB reports that he serves or has served on advisory boards for Cardax, CellProthera, Cereno Scientific, Elsevier Practice Update Cardiology, Level Ex, Medscape Cardiology, PhaseBio, PLx Pharma and Regado Biosciences. He is or was a member of the board of directors for Boston VA Research Institute, Society of Cardiovascular Patient Care, and TobeSoft. He is or was chair for the American Heart Association Quality Oversight Committee, and is or was on data monitoring committees for Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Cleveland Clinic (including for the ExCEED trial, funded by Edwards), Contego Medical (chair, PERFORMANCE 2), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo), and the Population Health Research Institute. He reports honoraria from the American College of Cardiology (senior associate editor, Clinical Trials and News, ACC.org; vice-chair, ACC Accreditation Committee), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee funded by Boehringer Ingelheim; AEGIS-II executive committee funded by CSL Behring), Belvoir Publications (editor in chief, Harvard Heart Letter), Duke Clinical Research Institute (clinical trial steering committees, including for the PRONOUNCE trial, funded by Ferring Pharmaceuticals), HMP Global (editor in chief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (guest editor and associate editor), K2P (cochair, interdisciplinary curriculum), Level Ex, Medtelligence/ReachMD (CME steering committees), MJH Life Sciences, Population Health Research Institute (for the COMPASS operations committee, publications committee, steering committee, and USA national coleader, funded by Bayer), Slack Publications (chief medical editor, Cardiology Today–Intervention), Society of Cardiovascular Patient Care (secretary/treasurer), WebMD (CME steering committees). He reports other relationships with Clinical Cardiology (deputy editor), NCDR-ACTION Registry Steering Committee (chair), and VA CART Research and Publications Committee (chair). He reports research funding from Abbott, Afimmune, Amarin, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Cardax, Chiesi, CSL Behring, Eisai, Ethicon, Ferring Pharmaceuticals, Forest Laboratories, Fractyl, Idorsia, Ironwood, Ischemix, Lexicon, Lilly, Medtronic, Pfizer, PhaseBio, PLx Pharma, Regeneron, Roche, Sanofi Aventis, Synaptic, and The Medicines Company. He reports royalties from Elsevier (editor, Cardiovascular Intervention: A Companion to Braunwald’s Heart Disease). He is or was a site coinvestigator for Biotronik, Boston Scientific, CSI, St. Jude Medical (now Abbott), and Svelte. He is or was a trustee for the American College of Cardiology. He reports unfunded research for FlowCo, Merck, Novo Nordisk, and Takeda. HR, JCL-T, KW, and VB are full-time employees of Fractyl Laboratories and may hold Fractyl stock and/or stock options. GC has received research grant support from Boston Scientific and Apollo and is on the advisory board for Cook Medical, Olympus, and Ethicon. RH has received funding/grant support/honorarium for consultancy from Cook Endoscopy, Pentax Europe, Medtronic, C2 Therapeutics, and Fractyl Laboratories to support research infrastructure. EG has received consulting fees from Fractyl Laboratories Inc, Apollo Endosurgery, and Medtronic. MGN has received honorarium for consultancy from Fractyl Laboratories, GI Windows, GI Dynamics, Apollo, and for speaker bureaus for Ethicon, Medtronic, and Olympus. GPA has been a consultant and advisory board member for Agios Pharmaceuticals, Amryt Pharma, AstraZeneca, GlaxoSmithKline and Pfizer. AR has received grant support from Norgine, Fujifilm, Boston Scientific and ERBE, and served as a member of advisory boards for Medtronic, Boston Scientific, EndoStart, EndoKey, Alfasigma and FujiFilm. AJM has received honorarium for consultancy from Fractyl Laboratories and Cook Medical. ACGvB, BH, RB, AH, MDC and NSS have nothing to disclose. AJS has been a consultant for Conatus, Gilead, Elsevier, Echosens, Malinckrodt, Immuron, Intercept, Pfizer, Salix, Uptodate, Boehringer, Ingelhiem, Novartis, Nimbus, Nitto Denko, Hemoshear, Lilly, Novo Nordisk, Fractyl Laboratories, Allergan, Chemomab, Affimmune, Teva, Ardelyx, Terns, ENYO, Birdrock, Albireo, Sanofi, Jannsen, Takeda, Zydus, BASF, Amra, Perspectum, OWL, Poxel, Servier, Second Genome, General Electric, and 89Bio. He is a stock/shareholder at Exhalenz Stock, Akarna, Durect, Indalo and Tiziana. He has received grant/research support from Novartis, Merck, Galectin, Bristol Myers, Merck, Sequana, Boehringer Ingelheim, Echosense, Salix, Malinckrodt, Cumberland, and Gilead.JJGHMB has received research support from Fractyl Laboratories for IRB-based studies and has received a consultancy fee for a single advisory board meeting for Fractyl Laboratories in September 2019.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous