

Purulent pericarditis-induced intracardiac perforation and infective endocarditis due to Parvimonas micra: a case report
- PMID: 33598614
- PMCID: PMC7873805
- DOI: 10.1093/ehjcr/ytaa528
Purulent pericarditis-induced intracardiac perforation and infective endocarditis due to Parvimonas micra: a case report
Abstract
Background: Purulent pericarditis, a rare disease with a high associated mortality rate in patients without adequate treatment, can cause serious complications, such as perforation of the surrounding tissue and organs. Parvimonas micra is a very rare cause of purulent pericarditis.
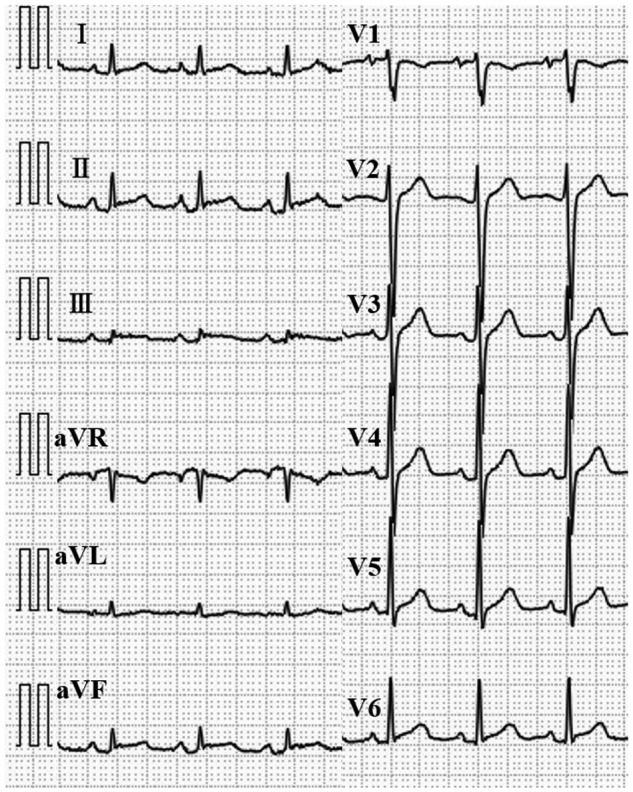
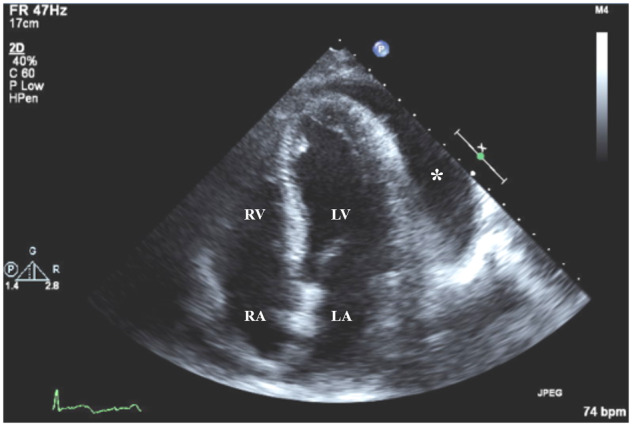
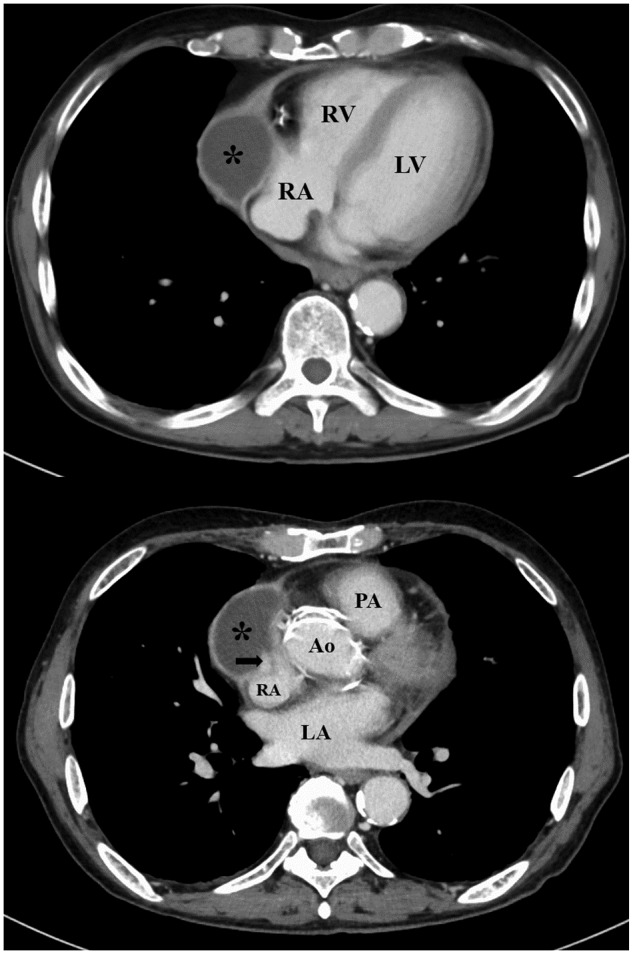
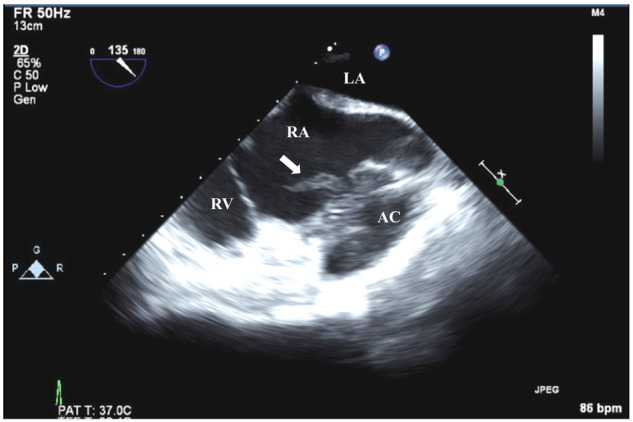
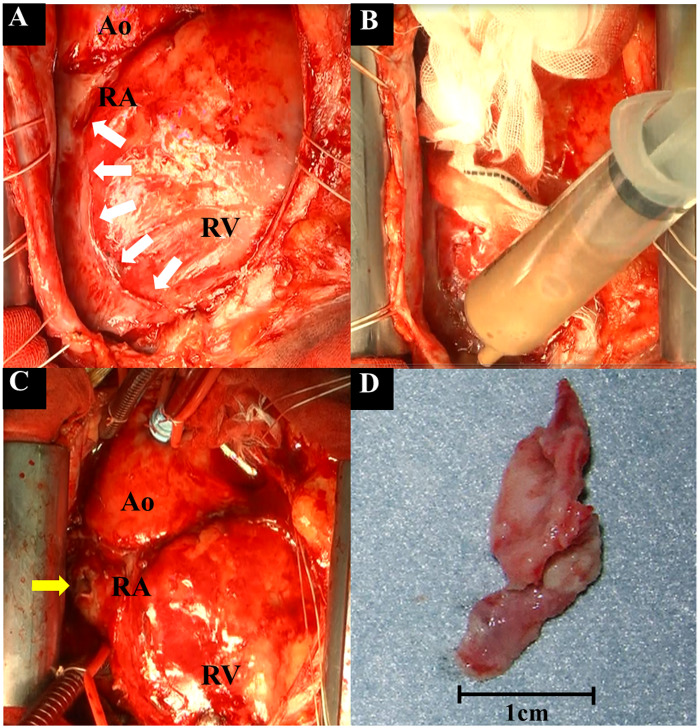
Case summary: A 70-year-old male patient presented to our emergency room with chest pain of 10 days' duration. An electrocardiogram showed ST-segment elevation and PR-segment depression on multiple leads. A transthoracic echocardiogram showed normal left ventricular function and a large amount of pericardial effusion. Acute pericarditis was diagnosed, and anti-inflammatory drug therapy was initiated. Due to the lack of improvement in the symptoms, pericardiocentesis was performed on Day 8 and revealed about 800 cc of the bloody fluid. Parvimonas micra was detected in a culture of the pericardial effusion and blood. Although intravenous antibiotic therapy was initiated for purulent pericarditis, his fever persisted. Computed tomography of the chest performed on Day 14 showed an abscess cavity in the pericardial space around the right atrium (RA). Furthermore, transoesophageal echocardiography revealed vegetation in the RA. Emergency surgery confirmed the presence of vegetation and minor perforation of the RA with communication to the abscess cavity. After surgical therapy, the patient clinically improved and was discharged on Day 51.
Discussion: In cases of acute pericarditis, purulent pericarditis should be considered if clinical improvement is not observed after initial treatment with anti-inflammatory drugs. Once the diagnosis of purulent pericarditis is made, aggressive source control is necessary for improved clinical outcomes.
Keywords: Case report; Infective endocarditis; Intracardiac perforation; Parvimonas micra; Purulent pericarditis.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Imazio M, Cecchi E, Demichelis B, Ierna S, Demarie D, Ghisio A. et al. Indicators of poor prognosis of acute pericarditis. Circulation 2007;115:2739–2744. - PubMed
-
- Parikh SV, Memon N, Echols M, Shah J, McGuire DK, Keeley EC.. Purulent pericarditis: report of 2 cases and review of the literature. Medicine (Baltimore) 2009;88:52–65. - PubMed
-
- Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del ZF. et al. 2015 ESC Guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC) Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J 2015;36:3075–3128. - PubMed
-
- Imazio M, Adler Y.. Management of pericardial effusion. Eur Heart J 2013;34:1186–1197. - PubMed
-
- Brook L. Pericarditis caused by anaerobic bacteria. Int J Antimicrob Agents 2009;33:279–300. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials