

Musculoskeletal involvement of COVID-19: review of imaging
- PMID: 33598718
- PMCID: PMC7889306
- DOI: 10.1007/s00256-021-03734-7
Musculoskeletal involvement of COVID-19: review of imaging
Abstract
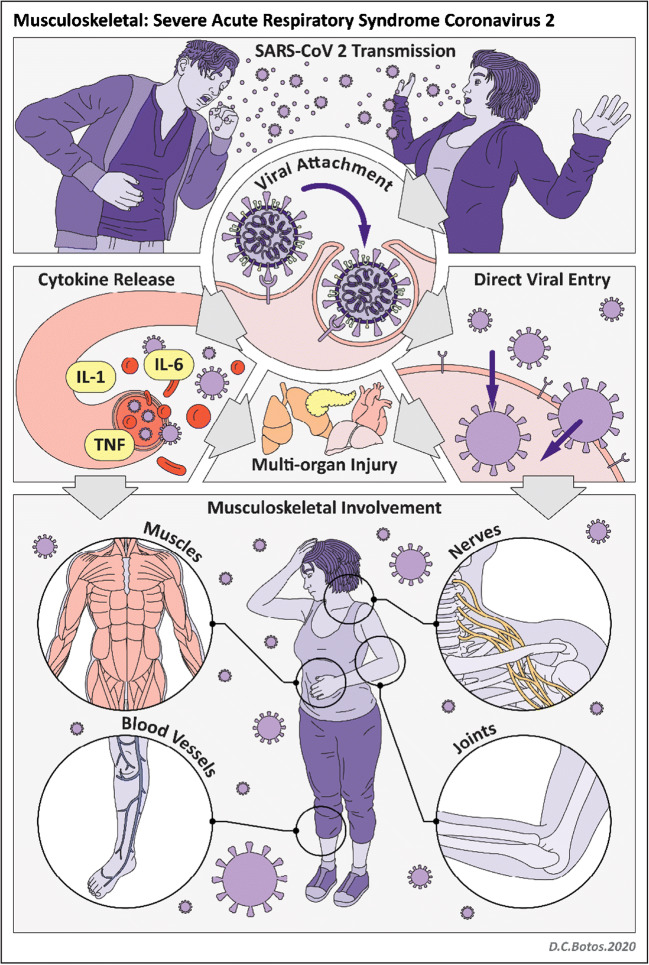
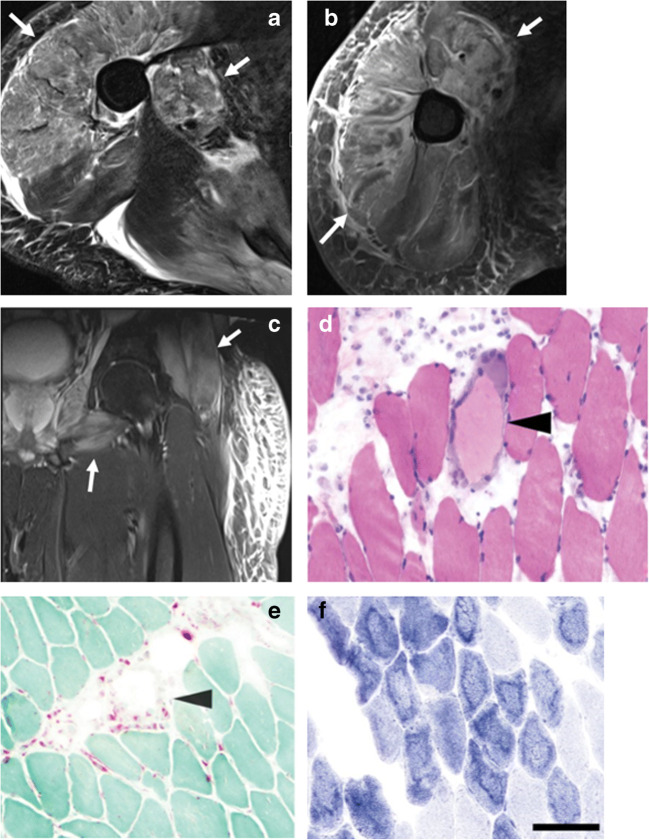
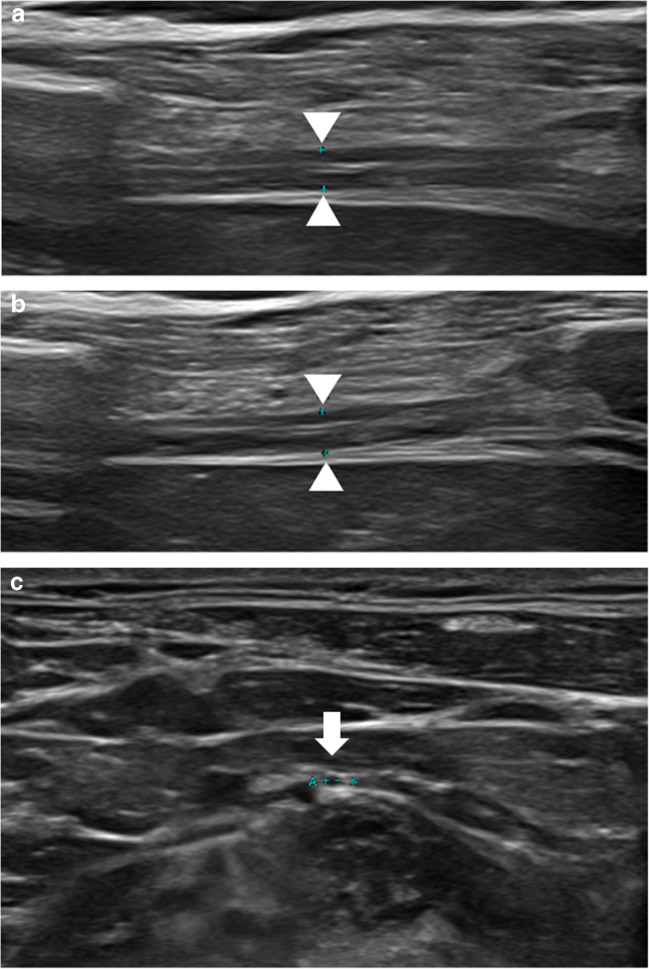
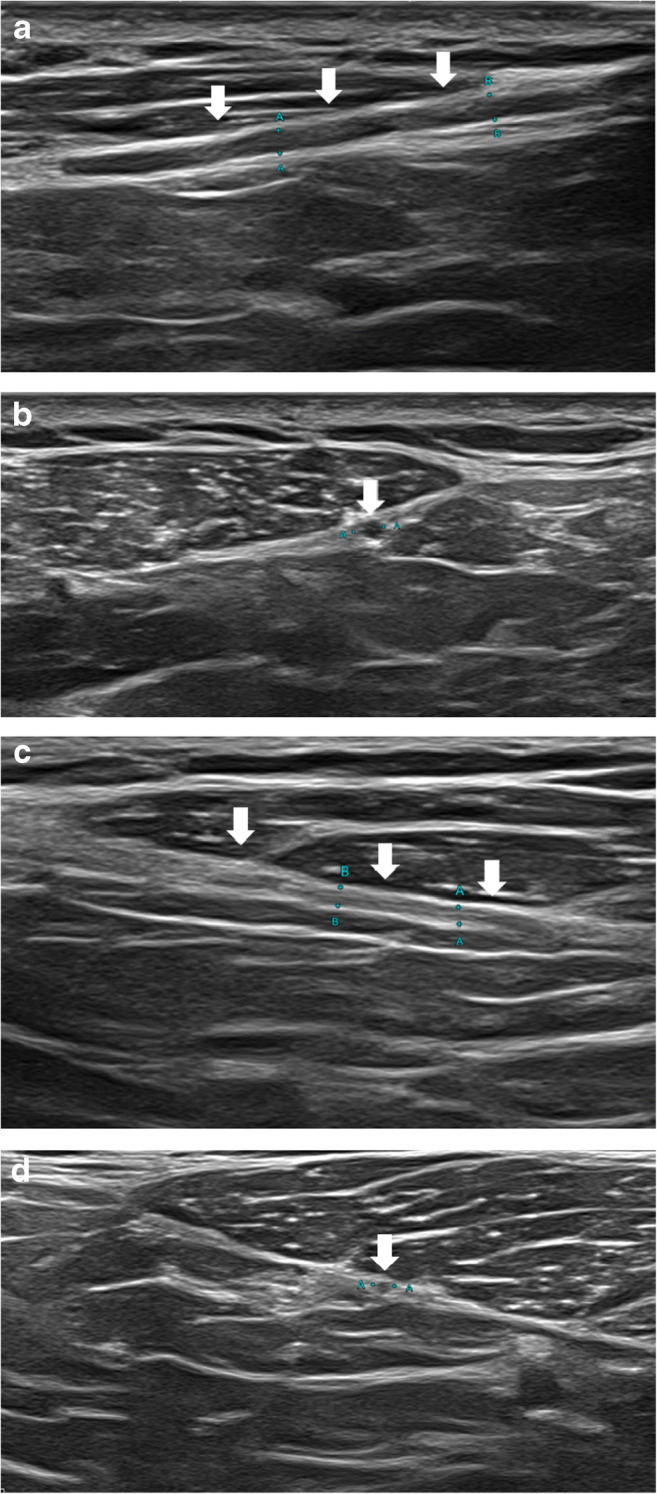
The global pandemic of coronavirus disease 2019 (COVID-19) has revealed a surprising number of extra-pulmonary manifestations of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. While myalgia is a common clinical feature of COVID-19, other musculoskeletal manifestations of COVID-19 were infrequently described early during the pandemic. There have been emerging reports, however, of an array of neuromuscular and rheumatologic complications related to COVID-19 infection and disease course including myositis, neuropathy, arthropathy, and soft tissue abnormalities. Multimodality imaging supports diagnosis and evaluation of musculoskeletal disorders in COVID-19 patients. This article aims to provide a first comprehensive summary of musculoskeletal manifestations of COVID-19 with review of imaging.
Keywords: COVID-19; MR; Musculoskeletal; Neuromuscular; SARS-CoV-2; Ultrasound.
© 2021. ISS.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Johns Hopkins University & Medicine Coronavirus Resource Center. https://coronavirus.jhu.edu/map.html. Accessed 1/10/21
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
