

Age-Related Trajectories of Cardiovascular Risk and Use of Aspirin and Statin Among U.S. Adults Aged 50 or Older, 2011-2018
- PMID: 33598936
- PMCID: PMC9869399
- DOI: 10.1111/jgs.17038
Age-Related Trajectories of Cardiovascular Risk and Use of Aspirin and Statin Among U.S. Adults Aged 50 or Older, 2011-2018
Abstract
Objectives: To examine age-related trajectories of cardiovascular risk and use of aspirin and statin among U.S. adults aged 50 or older.
Design: Repeated cross-sectional study using data from 2011 to 2018 National Health and Nutrition Examination Surveys.
Setting: Nationally representative health interview survey in the United States.
Participants: Non-institutionalized adults aged 50 years and older (n = 11,392 unweighted).
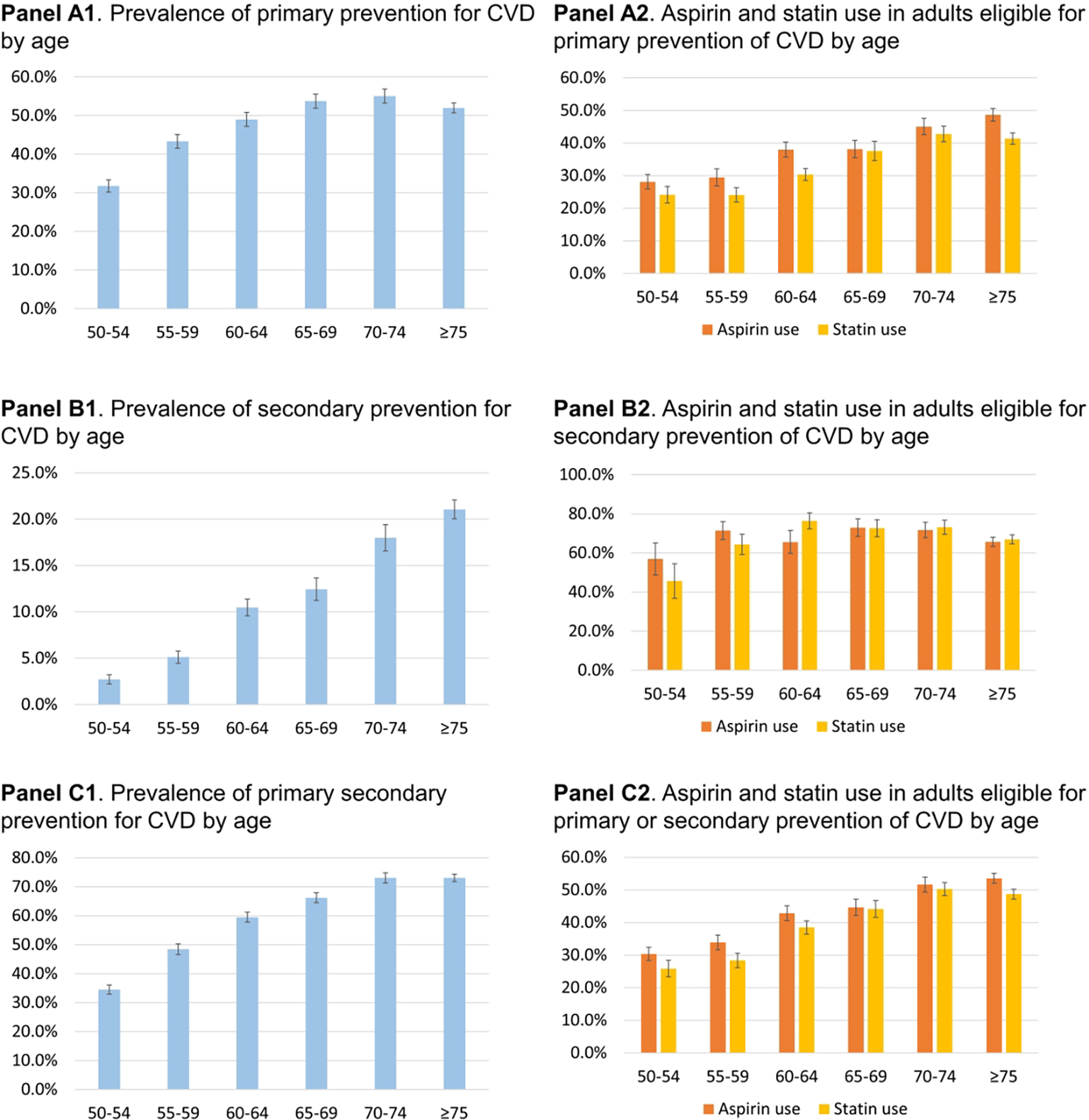
Measurements: Primary prevention was defined as the prevention of a first cardiovascular event including coronary heart disease, angina/angina pectoris, heart attack, or stroke, whereas secondary prevention was defined as those with a history of these clinical conditions. Medication use was determined by self-report; aspirin use included dose and frequency, and statin use included generic names, days of prescription fills, and indications. We examined linear trends between age and each medication use, after controlling for period, sex, and race/ethnicity.
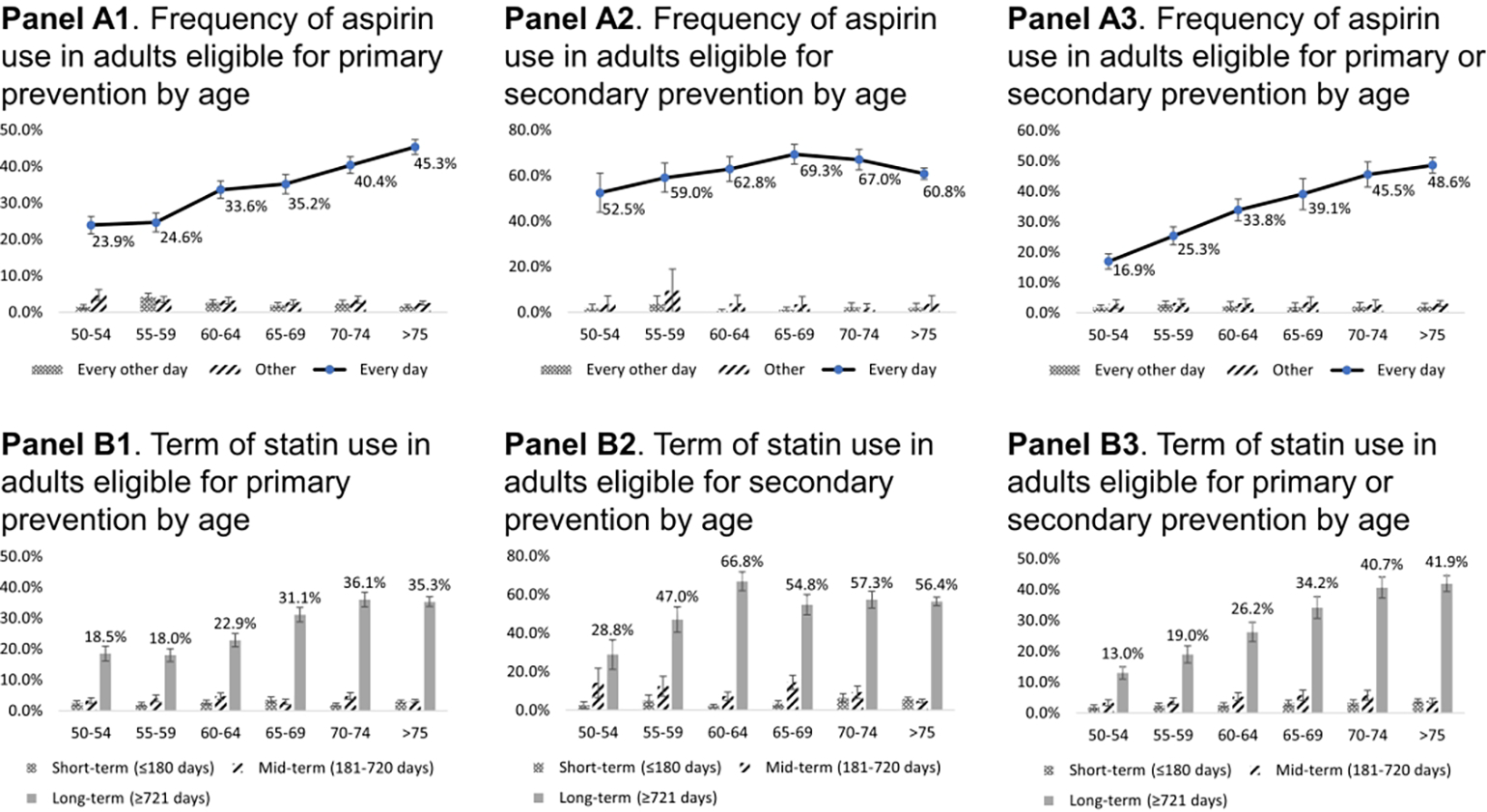
Results: Prevalence of those eligible for primary prevention treatment increased with age from 31.8% in ages 50-54 to 52.0% in ages ≥75 (p < 0.001). Similarly, those eligible for secondary prevention treatment increased with age from 2.7% in ages 50-54 to 21.1% in ages ≥75 (p < 0.001). Low-dose daily aspirin use increased with age (p < 0.001), and 45.3% of adults aged ≥75 took low-dose aspirin daily for primary prevention. Statin use also increased with age (p < 0.001), and 56.4% of adults aged ≥75 had long-term statin use for secondary prevention.
Conclusion: While adults aged ≥75 do not benefit from the use of aspirin to prevent the first CVD, many continue to take aspirin on a regular basis. In spite of the clear benefit of statin use to prevent a subsequent CVD event, many older adults in this risk category are not taking a statin. Further education and guidance for both healthcare providers and older adults regarding the appropriate use of aspirin and statins to prevent CVD is needed.
Keywords: aspirin; cardiovascular; pharmaco-epidemiology; statin.
© 2021 The American Geriatrics Society.
Conflict of interest statement
Figures
References
-
- Semb AG, Ikdahl E, Wibetoe G, Crowson C, Rollefstad S. Atherosclerotic cardiovascular disease prevention in rheumatoid arthritis. Nat Rev Rheumatol. 2020;16(7):361–379. - PubMed
-
- World Health Organization. Cardiovascular dieases. 2020; https://www.who.int/health-topics/cardiovascular-diseases/#tab=tab_1. Accessed November 5, 2020.
-
- Centers for Disease Control and Prevention. Heart disease. 2020; https://www.cdc.gov/heartdisease/facts.htm. Accessed November 5, 2020.
-
- Coll PP, Roche V, Olsen JS, Voit JH, Bowen E, Kumar M. The Prevention of Cardiovascular Disease in Older Adults. J Am Geriatr Soc. 2020;68(5):1098–1106. - PubMed
-
- Peters AT, Mutharasan RK. Aspirin for Prevention of Cardiovascular Disease. JAMA. 2020;323(7):676–676. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
