

Long-term outcomes in young patients with atrioventricular block of unknown aetiology
- PMID: 33599276
- PMCID: PMC8169155
- DOI: 10.1093/eurheartj/ehab060
Long-term outcomes in young patients with atrioventricular block of unknown aetiology
Erratum in
-
Corrigendum to: Long-term outcomes in young patients with atrioventricular block of unknown aetiology.Eur Heart J. 2021 Jun 1;42(21):2112. doi: 10.1093/eurheartj/ehab155. Eur Heart J. 2021. PMID: 33787884 Free PMC article. No abstract available.
Abstract
Aims: Atrioventricular block (AVB) of unknown aetiology is rare in the young, and outcome in these patients is unknown. We aimed to assess long-term morbidity and mortality in young patients with AVB of unknown aetiology.
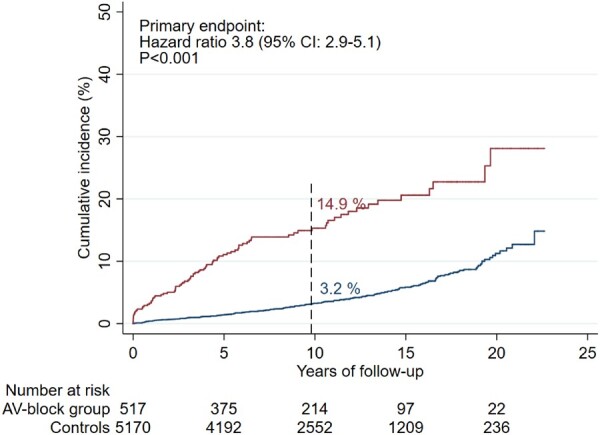
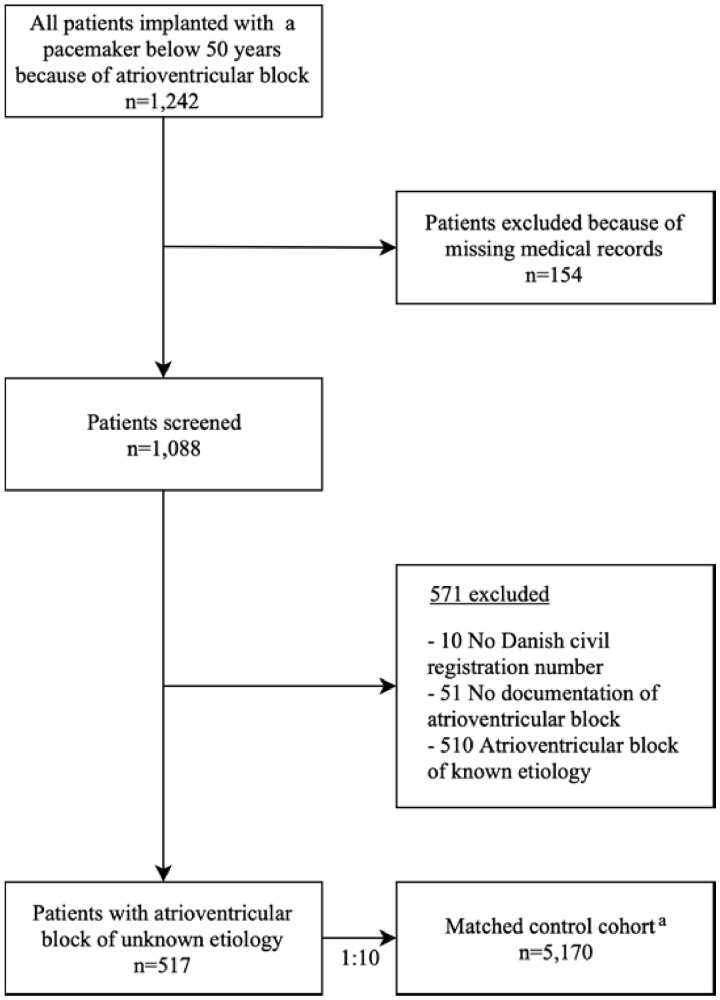
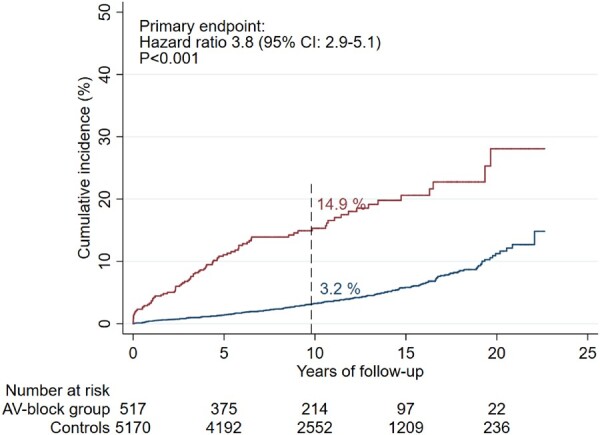
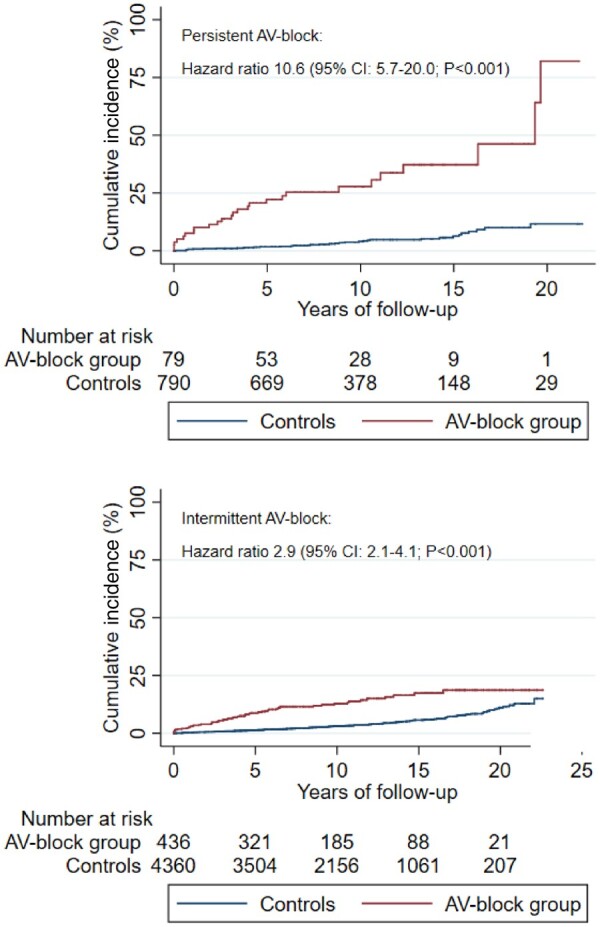
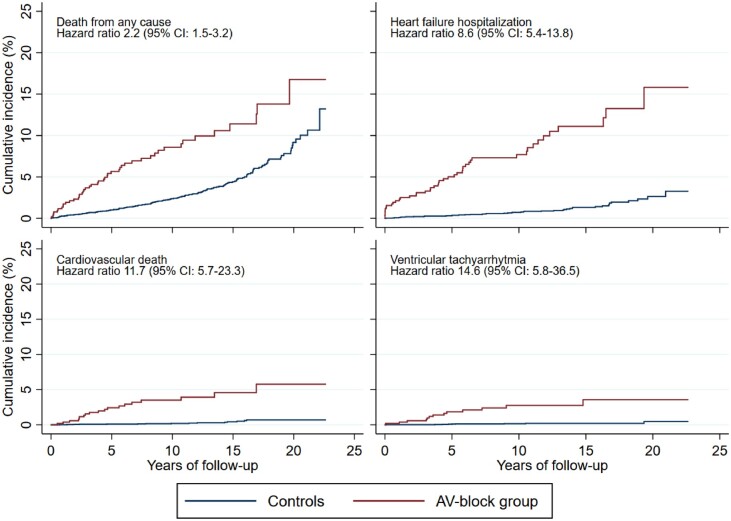
Methods and results: We identified all Danish patients younger than 50 years receiving a first pacemaker due to AVB between January 1996 and December 2015. By reviewing medical records, we included patients with AVB of unknown aetiology. A matched control cohort was established. Follow-up was performed using national registries. The primary outcome was a composite endpoint consisting of death, heart failure hospitalization, ventricular tachyarrhythmia, and cardiac arrest with successful resuscitation. We included 517 patients, and 5170 controls. Median age at first pacemaker implantation was 41.3 years [interquartile range (IQR) 32.7-46.2 years]. After a median follow-up of 9.8 years (IQR 5.7-14.5 years), the primary endpoint had occurred in 14.9% of patients and 3.2% of controls [hazard ratio (HR) 3.8; 95% confidence interval (CI) 2.9-5.1; P < 0.001]. Patients with persistent AVB at time of diagnosis had a higher risk of the primary endpoint (HR 10.6; 95% CI 5.7-20.0; P < 0.001), and risk was highest early in the follow-up period (HR 6.8; 95% CI 4.6-10.0; P < 0.001, during 0-5 years of follow-up).
Conclusion: Atrioventricular block of unknown aetiology presenting before the age of 50 years and treated with pacemaker implantation was associated with a three- to four-fold higher rate of the composite endpoint of death or hospitalization for heart failure, ventricular tachyarrhythmia, or cardiac arrest with successful resuscitation. Patients with persistent AVB were at higher risk. These findings warrant improved follow-up strategies for young patients with AVB of unknown aetiology.
Keywords: Atrioventricular block; Follow-up; Long-term outcomes; Pacemaker implantation; Unknown aetiology; Young.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Poor prognosis in young patients with atrioventricular block of unknown aetiology: who is to blame? The physician or the pacemaker?Eur Heart J. 2021 Jun 1;42(21):2069-2071. doi: 10.1093/eurheartj/ehab130. Eur Heart J. 2021. PMID: 33693637 No abstract available.
References
-
- Danish Pacemaker and ICD Register. Danish Pacemaker and ICD Register Annual report 2015. https://ssl.icddata.dk/download/Danish_Pacemaker_and_ICD_Register_Annual....
-
- Udo EO, van Hemel NM, Zuithoff NP, Doevendans PA, Moons KG. Prognosis of the bradycardia pacemaker recipient assessed at first implantation: a nationwide cohort study. Heart 2013;99:1573–1578. - PubMed
-
- Lenegre J. Etiology and pathology of bilateral bundle branch block in relation to complete heart block. Prog Cardiovasc Dis 1964;6:409–444. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
