

Association of Bone Metastatic Burden With Survival Benefit From Prostate Radiotherapy in Patients With Newly Diagnosed Metastatic Prostate Cancer: A Secondary Analysis of a Randomized Clinical Trial
- PMID: 33599706
- PMCID: PMC7893550
- DOI: 10.1001/jamaoncol.2020.7857
Association of Bone Metastatic Burden With Survival Benefit From Prostate Radiotherapy in Patients With Newly Diagnosed Metastatic Prostate Cancer: A Secondary Analysis of a Randomized Clinical Trial
Abstract
Importance: Prostate radiotherapy (RT) improves survival in men with low-burden metastatic prostate cancer. However, owing to the dichotomized nature of metastatic burden criteria, it is not clear how this benefit varies with bone metastasis counts and metastatic site.
Objective: To evaluate the association of bone metastasis count and location with survival benefit from prostate RT.
Design, setting, and participants: This exploratory analysis of treatment outcomes based on metastatic site and extent as determined by conventional imaging (computed tomography/magnetic resonance imaging and bone scan) evaluated patients with newly diagnosed metastatic prostate cancer randomized within the STAMPEDE trial's metastasis M1 RT comparison. The association of baseline bone metastasis counts with overall survival (OS) and failure-free survival (FFS) was assessed using a multivariable fractional polynomial interaction procedure. Further analysis was conducted in subgroups.
Interventions: Patients were randomized to receive either standard of care (androgen deprivation therapy with or without docetaxel) or standard of care and prostate RT.
Main outcomes and measures: The primary outcomes were OS and FFS.
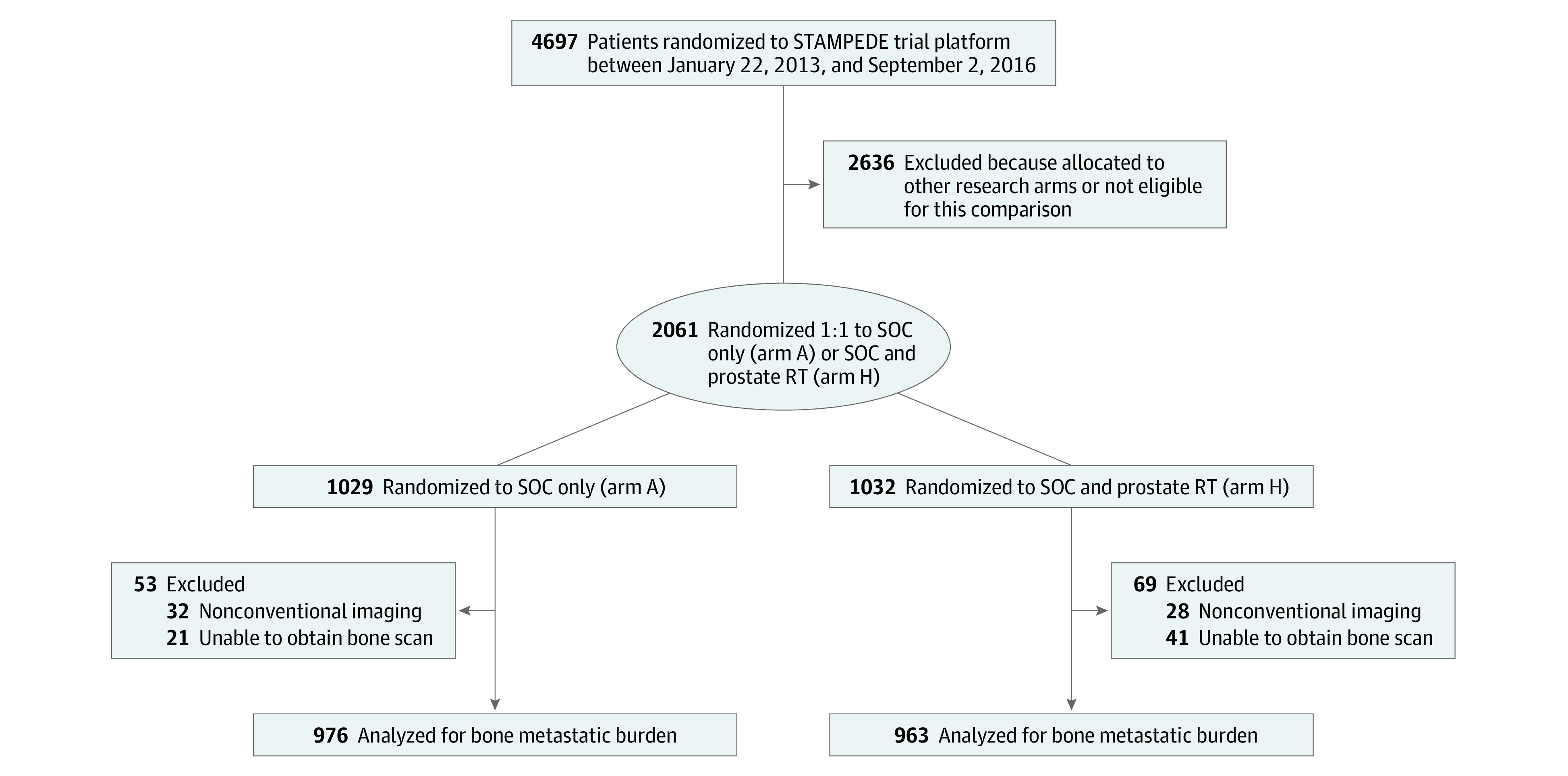
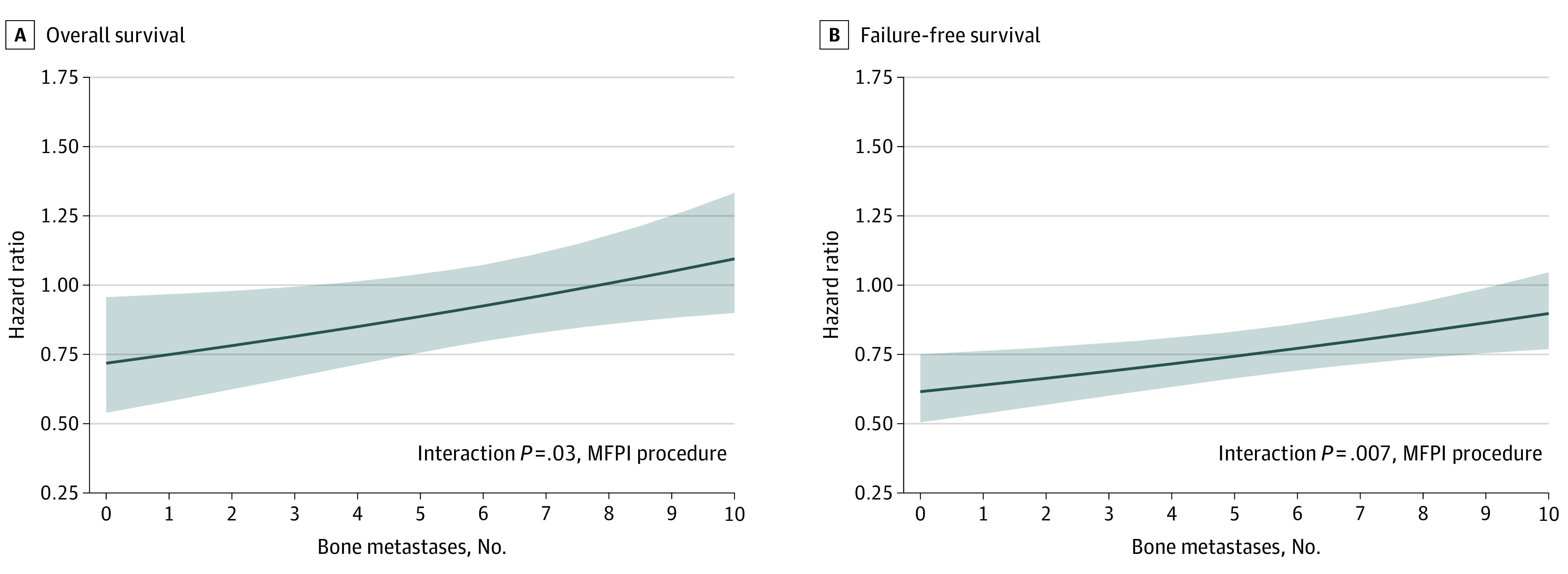
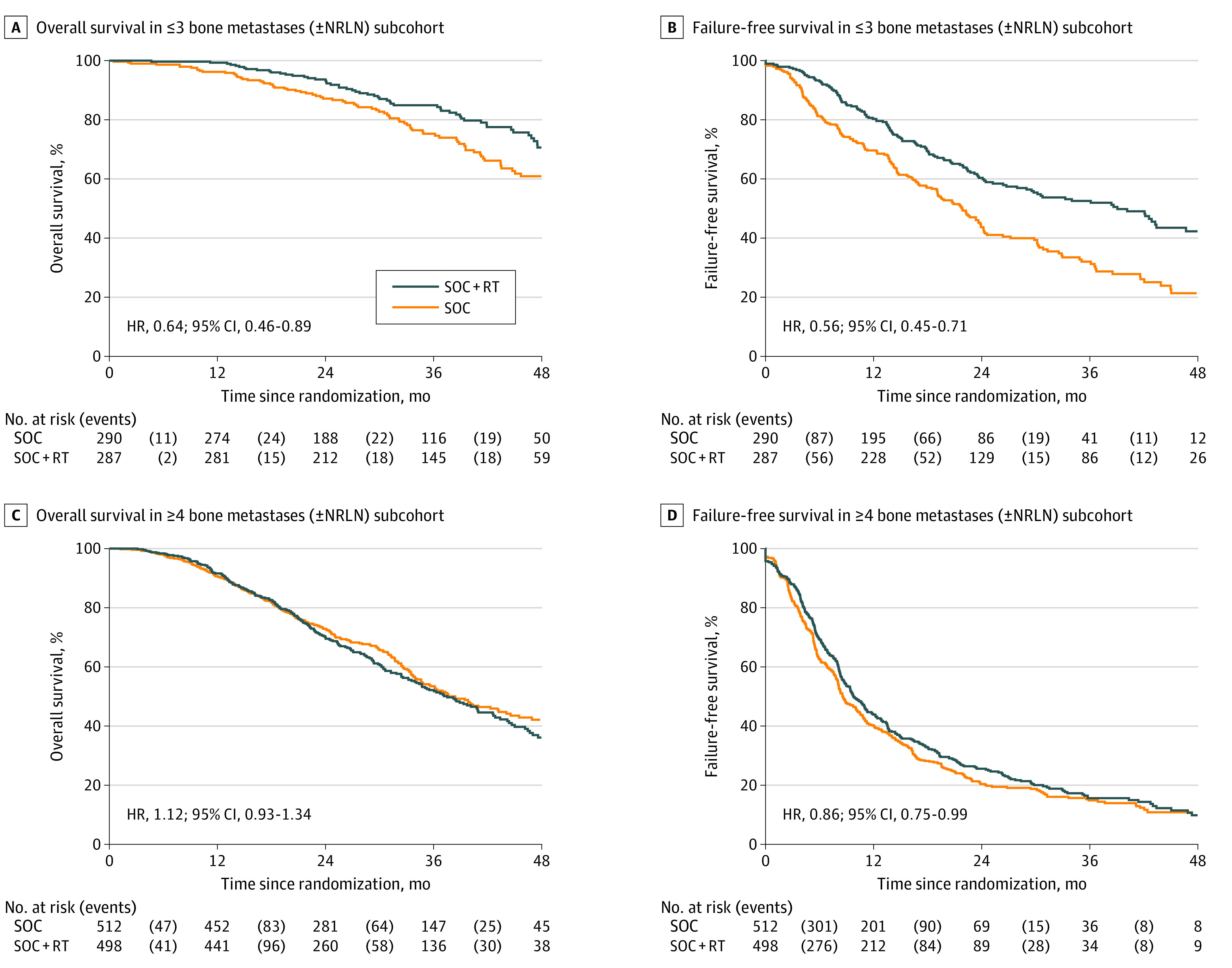
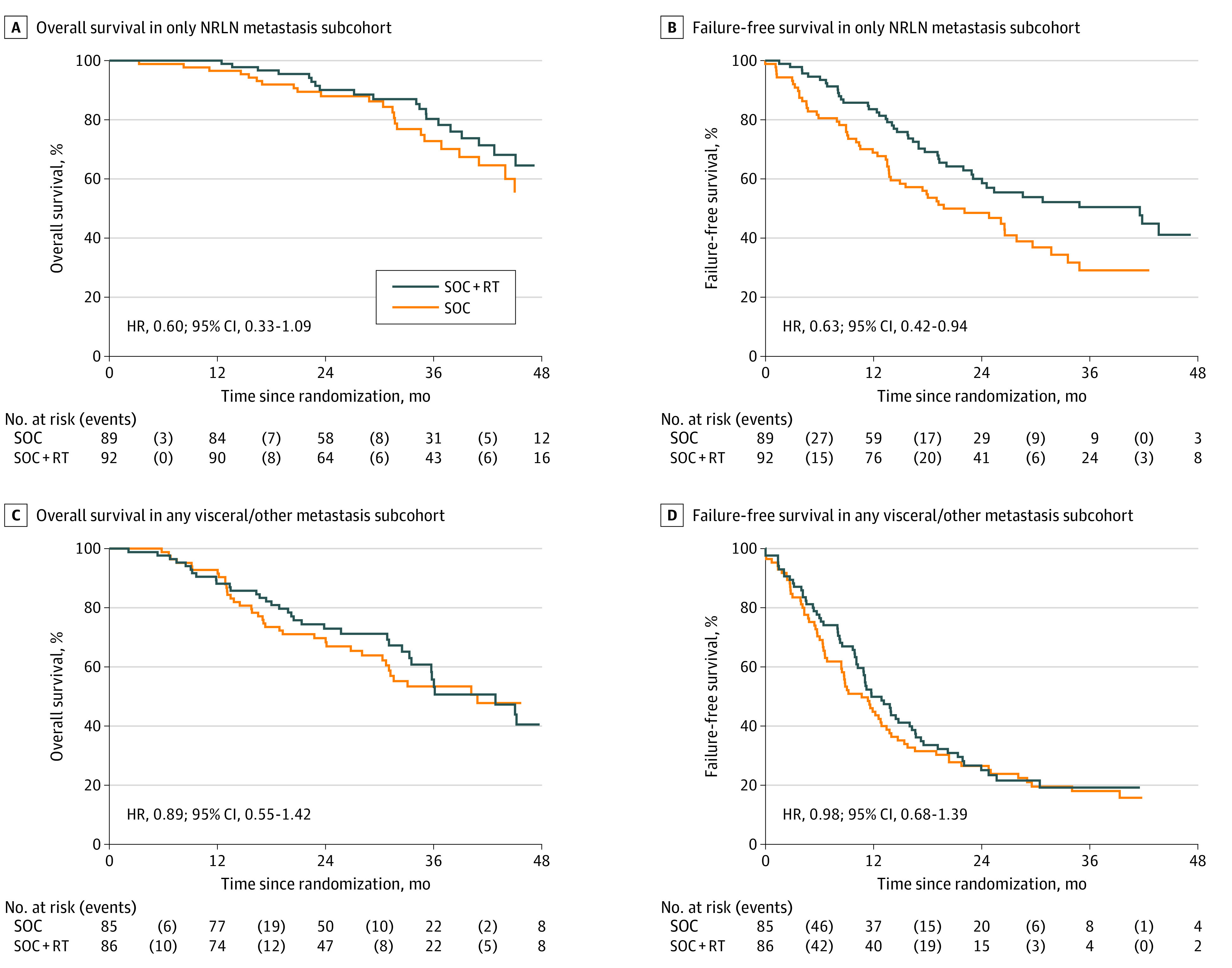
Results: A total of 1939 of 2061 men were included (median [interquartile range] age, 68 [63-73] years); 1732 (89%) had bone metastases. Bone metastasis counts were associated with OS and FFS benefit from prostate RT. Survival benefit decreased continuously as the number of bone metastases increased, with benefit most pronounced up to 3 bone metastases. A plot of estimated treatment effect indicated that the upper 95% CI crossed the line of equivalence (hazard ratio [HR], 1) above 3 bone metastases without a detectable change point. Further analysis based on subgroups showed that the magnitude of benefit from the addition of prostate RT was greater in patients with low metastatic burden with only nonregional lymph nodes (M1a) or 3 or fewer bone metastases without visceral metastasis (HR for OS, 0.62; 95% CI, 0.46-0.83; HR for FFS, 0.57; 95% CI, 0.47-0.70) than among patients with 4 or more bone metastases or any visceral/other metastasis (HR for OS, 1.08; 95% CI, 0.91-1.28; interaction P = .003; HR for FFS, 0.87; 95% CI, 0.76-0.99; interaction P = .002).
Conclusions and relevance: In this exploratory analysis of a randomized clinical trial, bone metastasis count and metastasis location based on conventional imaging were associated with OS and FFS benefit from prostate RT in M1 disease.
Trial registration: ClinicalTrials.gov Identifier: NCT00268476; ISRCTN.com Identifier: ISRCTN78818544.
Conflict of interest statement
Figures
Comment in
-
More Answers and More Questions About Radiotherapy for Metastatic Prostate Cancer.JAMA Oncol. 2021 Apr 1;7(4):563-564. doi: 10.1001/jamaoncol.2020.7708. JAMA Oncol. 2021. PMID: 33599702 No abstract available.
-
Urological Oncology: Prostate Cancer.J Urol. 2021 Jul;206(1):158-161. doi: 10.1097/JU.0000000000001814. Epub 2021 Apr 21. J Urol. 2021. PMID: 33881346 No abstract available.
References
-
- Parker CC, James ND, Brawley CD, et al. ; Systemic Therapy for Advanced or Metastatic Prostate cancer: Evaluation of Drug Efficacy (STAMPEDE) investigators . Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet. 2018;392(10162):2353-2366. doi: 10.1016/S0140-6736(18)32486-3 - DOI - PMC - PubMed
-
- Boevé LMS, Hulshof MCCM, Vis AN, et al. Effect on survival of androgen deprivation therapy alone compared to androgen deprivation therapy combined with concurrent radiation therapy to the prostate in patients with primary bone metastatic prostate cancer in a prospective randomised clinical trial: data from the HORRAD trial. Eur Urol. 2019;75(3):410-418. doi: 10.1016/j.eururo.2018.09.008 - DOI - PubMed
-
- National Comprehensive Cancer Network . NCCN Clinical Practice Guidelines in Oncology: prostate cancer. Version 2.2019. Accessed March 7, 2019. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
-
- Mottet N, Bellmunt J, Briers E, et al. ; members of the EAU–ESTRO–ESUR–SIOG Prostate Cancer Guidelines Panel . EAU–ESTRO–ESUR–SIOG guidelines on prostate cancer. Accessed March 13, 2019. https://uroweb.org/guideline/prostate-cancer/
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
