

Erythrocytosis in a Large Cohort of Trans Men Using Testosterone: A Long-Term Follow-Up Study on Prevalence, Determinants, and Exposure Years
- PMID: 33599731
- PMCID: PMC8118580
- DOI: 10.1210/clinem/dgab089
Erythrocytosis in a Large Cohort of Trans Men Using Testosterone: A Long-Term Follow-Up Study on Prevalence, Determinants, and Exposure Years
Abstract
Context: Erythrocytosis is a known side effect of testosterone therapy that can increase the risk of thromboembolic events.
Objectives: To study the prevalence and determinants in the development of erythrocytosis in trans men using testosterone.
Methods: A 20-year follow-up study in adult trans men who started testosterone therapy and had monitoring of hematocrit at our center (n = 1073).
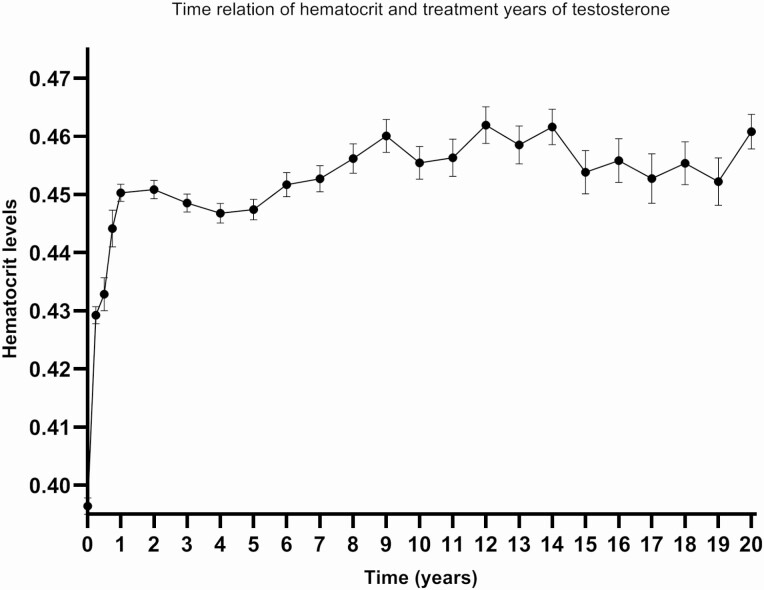
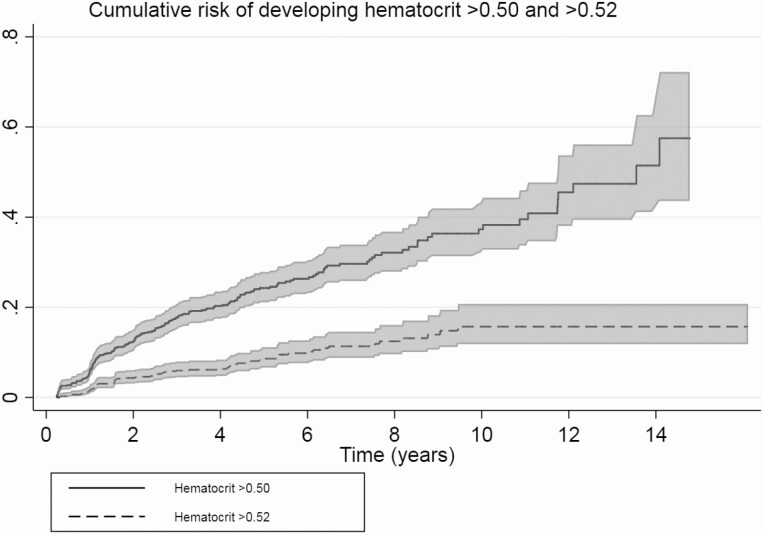
Results: Erythrocytosis occurred in 11% (hematocrit > 0.50 L/L), 3.7% (hematocrit > 0.52 L/L), and 0.5% (hematocrit > 0.54 L/L) of trans men. Tobacco use (odds ratio [OR] 2.2; 95% CI, 1.6-3.3), long-acting undecanoate injections (OR 2.9; 95% CI, 1.7-5.0), age at initiation of hormone therapy (OR 5.9; 95% CI, 2.8-12.3), body mass index (BMI) (OR 3.7; 95% CI, 2.2-6.2), and pulmonary conditions associated with erythrocytosis and polycythemia vera (OR 2.5; 95% CI, 1.4-4.4) were associated with hematocrit > 0.50 L/L. In the first year of testosterone therapy hematocrit increased most: 0.39 L/L at baseline to 0.45 L/L after 1 year. Although there was only a slight continuation of this increase in the following 20 years, the probability of developing erythrocytosis still increased (10% after 1 year, 38% after 10 years).
Conclusion: Erythrocytosis occurs in trans men using testosterone. The largest increase in hematocrit was seen in the first year, but also after the first years a substantial number of people present with hematocrit > 0.50 L/L. A reasonable first step in the care for trans men with erythrocytosis while on testosterone is to advise them to quit smoking, to switch to a transdermal administration route, and if BMI is high, to lose weight.
Keywords: erythrocytosis; gender dysphoria; hematocrit; hormone treatment; time relation; trans men.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Comment in
-
Response to Letter to the Editor From Laidlaw: "Erythrocytosis in a Large Cohort of Trans Men Using Testosterone: A Long-term Follow-up Study on Prevalence, Determinants, and Exposure Years".J Clin Endocrinol Metab. 2021 Oct 21;106(11):e4791-e4792. doi: 10.1210/clinem/dgab515. J Clin Endocrinol Metab. 2021. PMID: 34282457 Free PMC article. No abstract available.
-
Letter to the Editor From Laidlaw et al: "Erythrocytosis in a Large Cohort of Transgender Men Using Testosterone: A Long-term Follow-up Study on Prevalence, Determinants, and Exposure Years".J Clin Endocrinol Metab. 2021 Nov 19;106(12):e5275-e5276. doi: 10.1210/clinem/dgab514. J Clin Endocrinol Metab. 2021. PMID: 34297088 No abstract available.
-
Letter to the Editor from Giovanelli and Quinton: "Erythrocytosis in a Large Cohort of Trans Men Using Testosterone: a Long-Term Follow-up Study on Prevalence, Determinants, and Exposure Years".J Clin Endocrinol Metab. 2022 Jan 1;107(1):e440-e441. doi: 10.1210/clinem/dgab603. J Clin Endocrinol Metab. 2022. PMID: 34387315 No abstract available.
References
-
- Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
-
- Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2017; 102(11):3869-3903. - PubMed
-
- Irwig MS. Testosterone therapy for transgender men. Lancet Diabetes Endocrinol. 2017;5(4):301-311. - PubMed
-
- Irwig MS, Childs K, Hancock AB. Effects of testosterone on the transgender male voice. Andrology. 2017;5(1):107-112. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
