

Assessment of Combination Therapies vs Monotherapy for Erectile Dysfunction: A Systematic Review and Meta-analysis
- PMID: 33599772
- PMCID: PMC7893498
- DOI: 10.1001/jamanetworkopen.2020.36337
Assessment of Combination Therapies vs Monotherapy for Erectile Dysfunction: A Systematic Review and Meta-analysis
Abstract
Importance: Combining 2 first-line treatments for erectile dysfunction (ED) or initiating other modalities in addition to a first-line therapy may produce beneficial outcomes.
Objective: To assess whether different ED combination therapies were associated with improved outcomes compared with first-line ED monotherapy in various subgroups of patients with ED.
Data sources: Studies were identified through a systematic search in MEDLINE, Cochrane Library, and Scopus from inception of these databases to October 10, 2020.
Study selection: Randomized clinical trials or prospective interventional studies of the outcomes of combination therapy vs recommended monotherapy in men with ED were identified. Only comparative human studies, which evaluated the change from baseline of self-reported erectile function using validated questionnaires, that were published in any language were included.
Data extraction and synthesis: Data extraction and synthesis were performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline.
Main outcomes and measures: A meta-analysis was conducted that included randomized clinical trials that compared outcomes of combination therapy with phosphodiesterase type 5 (PDE5) inhibitors plus another agent vs PDE5 inhibitor monotherapy. Separate analyses were performed for the mean International Index of Erectile Function (IIEF) score change from baseline and the number of adverse events (AEs) by different treatment modalities and subgroups of patients.
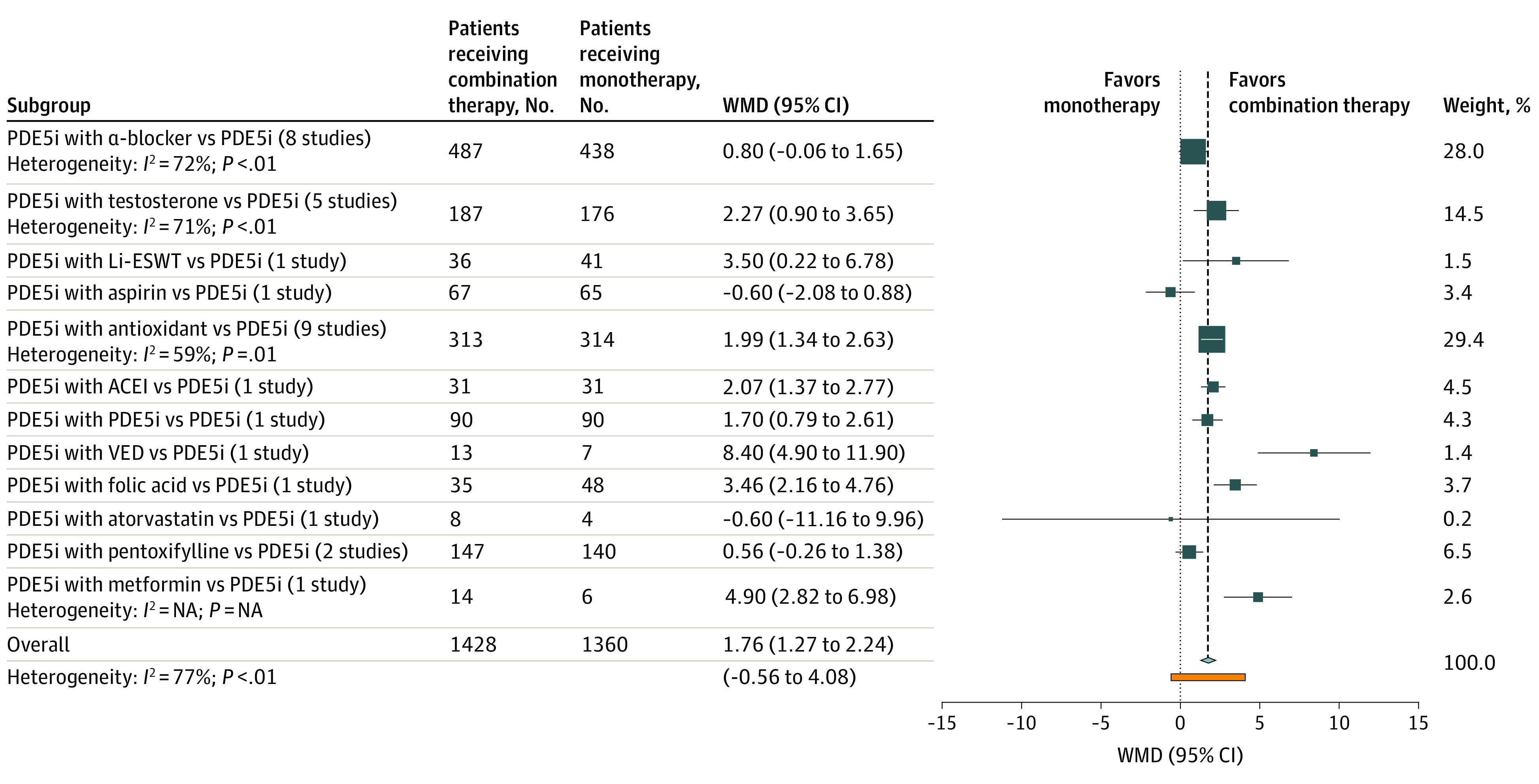
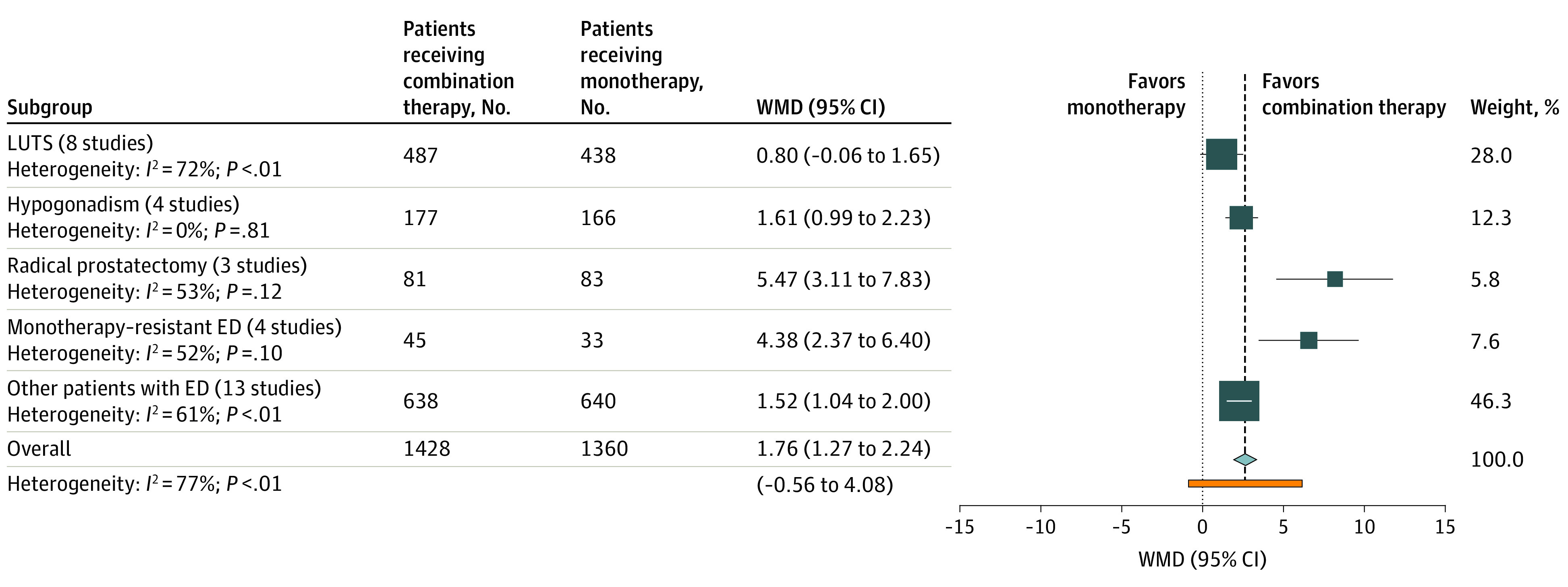
Results: A total of 44 studies included 3853 men with a mean (SD) age of 55.8 (11.9) years. Combination therapy compared with monotherapy was associated with a mean IIEF score improvement of 1.76 points (95% CI, 1.27-2.24; I2 = 77%; 95% PI, -0.56 to 4.08). Adding daily tadalafil, low-intensity shockwave therapy, vacuum erectile device, folic acid, metformin hydrochloride, or angiotensin-converting enzyme inhibitors was associated with a significant IIEF score improvement, but each measure was based on only 1 study. Specifically, the weighted mean difference (WMD) in IIEF score was 1.70 (95% CI, 0.79-2.61) for the addition of daily tadalafil, 3.50 (95% CI, 0.22-6.78) for the addition of low-intensity shockwave therapy, 8.40 (95% CI, 4.90-11.90) for the addition of a vacuum erectile device, 3.46 (95% CI, 2.16-4.76) for the addition of folic acid, 4.90 (95% CI, 2.82-6.98) for the addition of metformin hydrochloride and 2.07 (95% CI, 1.37-2.77) for the addition of angiotensin-converting enzyme inhibitors. The addition of α-blockers to PDE5 inhibitors was not associated with improvement in IIEF score (WMD, 0.80; 95% CI, -0.06 to 1.65; I2 = 72%). Compared with monotherapy, combination therapy was associated with improved IIEF score in patients with hypogonadism (WMD, 1.61; 95% CI, 0.99-2.23; I2 = 0%), monotherapy-resistant ED (WMD, 4.38; 95% CI, 2.37-6.40; I2 = 52%), or prostatectomy-induced ED (WMD, 5.47; 95% CI, 3.11-7.83; I2 = 53%). The treatment-related AEs did not differ between combination therapy and monotherapy (odds ratio, 1.10; 95% CI, 0.66-1.85; I2 = 78%). Despite multiple subgroup and sensitivity analyses, the levels of heterogeneity remained high.
Conclusions and relevance: This study found that combination therapy of PDE5 inhibitors and antioxidants was associated with improved ED without increasing the AEs. Treatment with PDE5 inhibitors and daily tadalafil, shockwaves, or a vacuum device was associated with additional improvement, but this result was based on limited data. These findings suggest that combination therapy is safe, associated with improved outcomes, and should be considered as a first-line therapy for refractory, complex, or difficult-to-treat cases of ED.
Conflict of interest statement
Figures
Comment in
-
Combination Therapies for Erectile Dysfunction-A Synergy of Modalities Holds the Key.JAMA Netw Open. 2021 Feb 1;4(2):e2037292. doi: 10.1001/jamanetworkopen.2020.37292. JAMA Netw Open. 2021. PMID: 33599768 No abstract available.
References
-
- Salonia A, Bettochi C, Carvalho J, et al. EAU guidelines on sexual and reproductive health. 2020. Accessed October 5, 2020. https://uroweb.org/guideline/sexual-and-reproductive-health/
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
