

Choosing the best algorithm among five thyroid nodule ultrasound scores: from performance to cytology sparing-a single-center retrospective study in a large cohort
- PMID: 33599836
- PMCID: PMC8270877
- DOI: 10.1007/s00330-021-07703-5
Choosing the best algorithm among five thyroid nodule ultrasound scores: from performance to cytology sparing-a single-center retrospective study in a large cohort
Abstract
Objective: Incidental diagnosis of thyroid nodules, and therefore of thyroid cancer, has definitely increased in recent years, but the mortality rate for thyroid malignancies remains very low. Within this landscape of overdiagnosis, several nodule ultrasound scores (NUS) have been proposed to reduce unnecessary diagnostic procedures. Our aim was to verify the suitability of five main NUS.
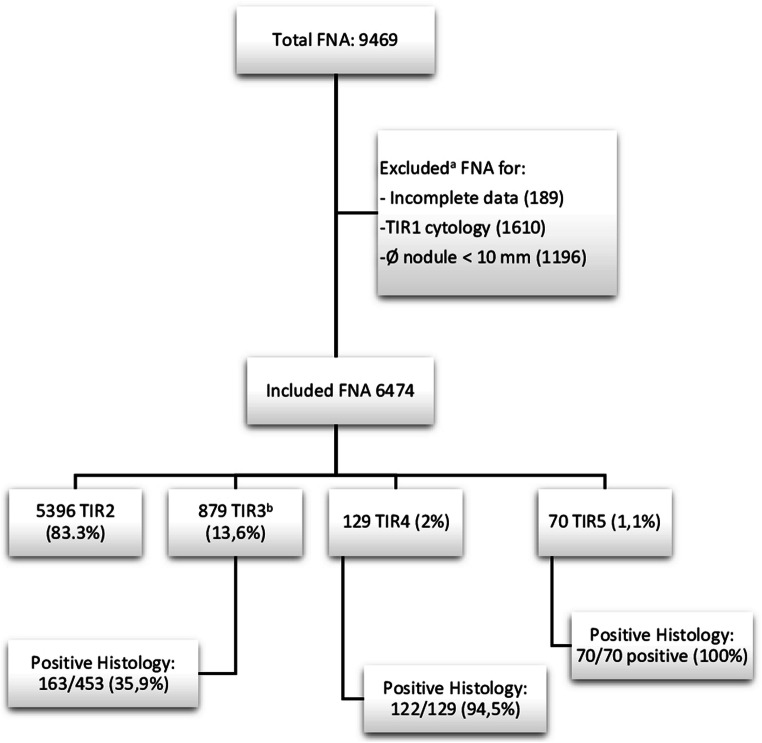
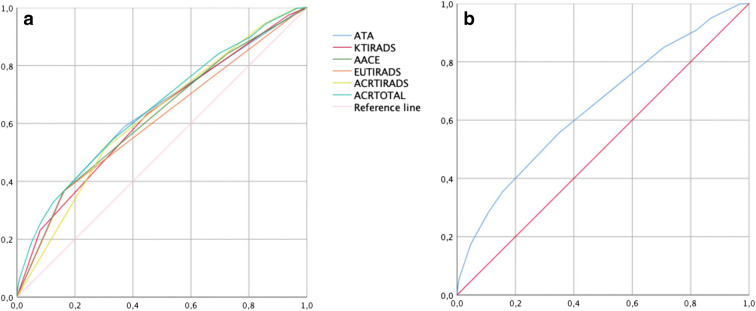
Methods: This single-center, retrospective, observational study analyzed a total number of 6474 valid cytologies. A full clinical and US description of the thyroid gland and nodules was performed. We retrospectively applied five available NUS: KTIRADS, ATA, AACE/ACE-AME, EUTIRADS, and ACRTIRADS. Thereafter, we calculated the sensitivity, specificity, PPV, and NPV, along with the number of possible fine-needle aspiration (FNA) sparing, according to each NUS algorithm and to clustering risk classes within three macro-groups (low, intermediate, and high risk).
Results: In a real-life setting of thyroid nodule management, available NUS scoring systems show good accuracy at ROC analysis (AUC up to 0.647) and higher NPV (up to 96%). The ability in FNA sparing ranges from 10 to 38% and reaches 44.2% of potential FNA economization in the low-risk macro-group. Considering our cohort, ACRTIRADS and AACE/ACE-AME scores provide the best compromise in terms of accuracy and spared cytology.
Conclusions: Despite several limitations, available NUS do appear to assist physicians in clinical practice. In the context of a common disease, such as thyroid nodules, higher accuracy and NPV are desirable NUS features. Further improvements in NUS sensitivity and specificity are attainable future goals to optimize nodule management.
Key points: • Thyroid nodule ultrasound scores do assist clinicians in real practice. • Ultrasound scores reduce unnecessary diagnostic procedures, containing indolent thyroid microcarcinoma overdiagnosis. • The variable malignancy risk of the "indeterminate" category negatively influences score's performance in real-life management of thyroid lesions.
Keywords: Biopsy, fine-needle; Cytology sparing; Thyroid imaging, reporting, and data system; Thyroid nodules; Ultrasonography.
© 2021. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
References
-
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26:1–133. doi: 10.1089/thy.2015.0020. - DOI - PMC - PubMed
-
- Cancer Stat Facts: Thyroid Cancer. https://seer.cancer.gov/statfacts/html/thyro.html
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
