

Machine Learning in Arrhythmia and Electrophysiology
- PMID: 33600229
- PMCID: PMC7899082
- DOI: 10.1161/CIRCRESAHA.120.317872
Machine Learning in Arrhythmia and Electrophysiology
Abstract
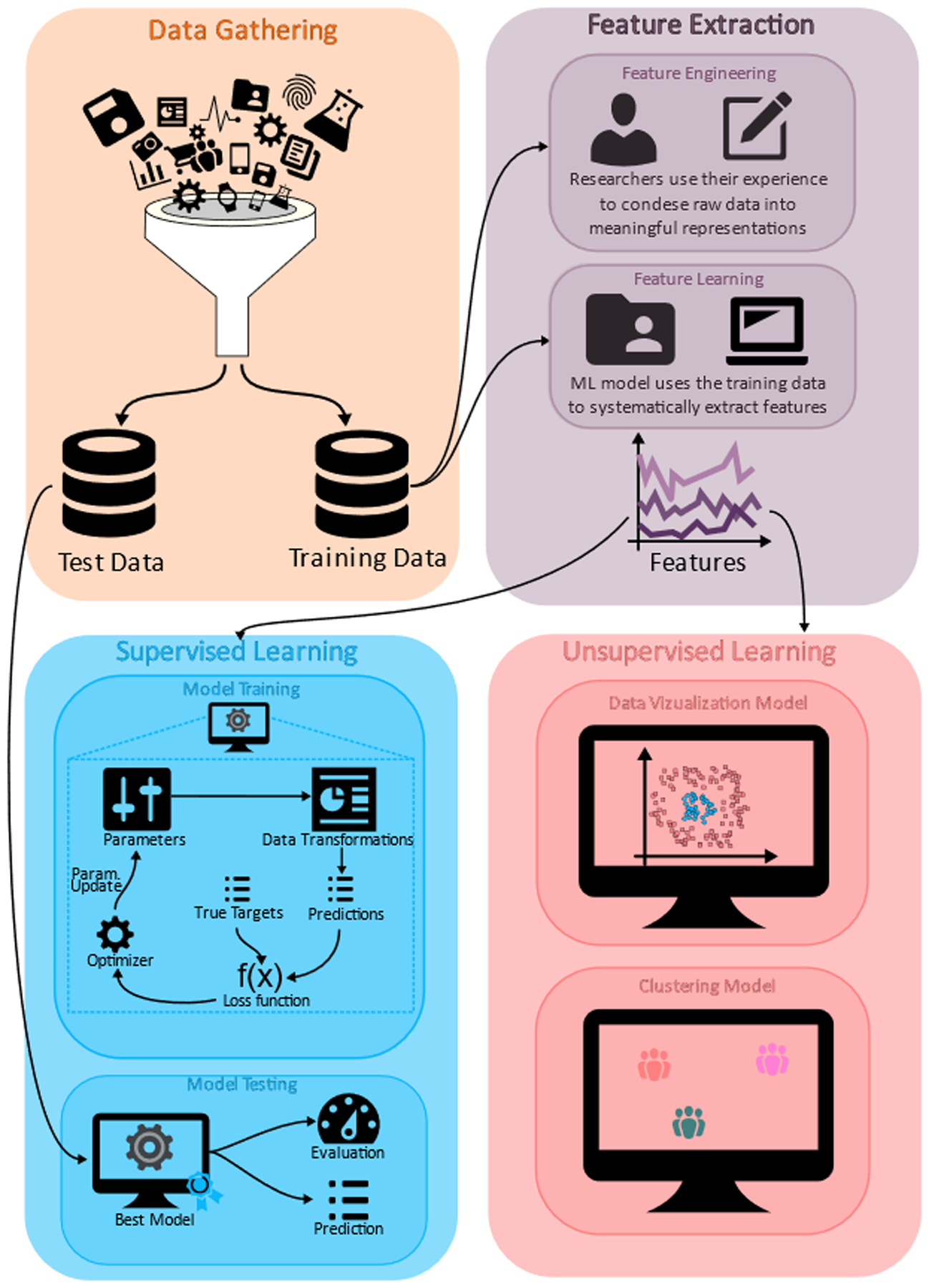
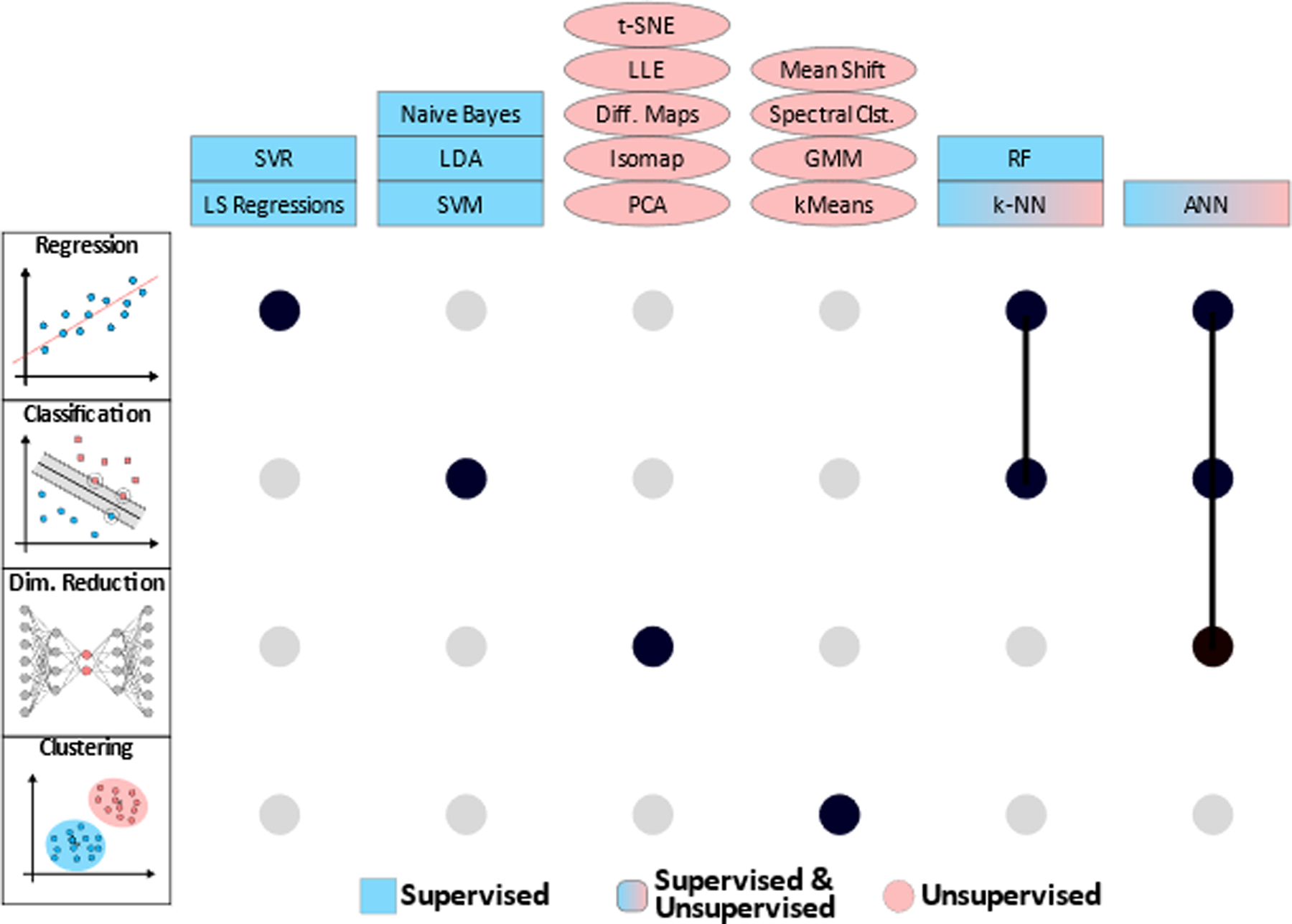
Machine learning (ML), a branch of artificial intelligence, where machines learn from big data, is at the crest of a technological wave of change sweeping society. Cardiovascular medicine is at the forefront of many ML applications, and there is a significant effort to bring them into mainstream clinical practice. In the field of cardiac electrophysiology, ML applications have also seen a rapid growth and popularity, particularly the use of ML in the automatic interpretation of ECGs, which has been extensively covered in the literature. Much lesser known are the other aspects of ML application in cardiac electrophysiology and arrhythmias, such as those in basic science research on arrhythmia mechanisms, both experimental and computational; in the development of better techniques for mapping of cardiac electrical function; and in translational research related to arrhythmia management. In the current review, we examine comprehensively such ML applications as they match the scope of this journal. The current review is organized in 3 parts. The first provides an overview of general ML principles and methodologies that will afford readers of the necessary information on the subject, serving as the foundation for inviting further ML applications in arrhythmia research. The basic information we provide can serve as a guide on how one might design and conduct an ML study. The second part is a review of arrhythmia and electrophysiology studies in which ML has been utilized, highlighting the broad potential of ML approaches. For each subject, we outline comprehensively the general topics, while reviewing some of the research advances utilizing ML under the subject. Finally, we discuss the main challenges and the perspectives for ML-driven cardiac electrophysiology and arrhythmia research.
Keywords: arrhythmias, cardiac; artificial intelligence; atrial fibrillation; electrophysiology; machine learning.
Figures


References
-
- Johnson KW, Torres Soto J, Glicksberg BS, Shameer K, Miotto R, Ali M, Ashley E, Dudley JT. Artificial Intelligence in Cardiology. J. Am. Coll. Cardiol 2018;71:2668–2679. - PubMed
-
- Krittanawong C, Zhang HJ, Wang Z, Aydar M, Kitai T. Artificial Intelligence in Precision Cardiovascular Medicine. J. Am. Coll. Cardiol 2017;69:2657–2664. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
