

Clinical and imaging features of congenital and acquired isolated inferior rectus muscle hypofunction
- PMID: 33601045
- PMCID: PMC8169540
- DOI: 10.1016/j.jaapos.2020.09.007
Clinical and imaging features of congenital and acquired isolated inferior rectus muscle hypofunction
Abstract
Background: Inferior rectus (IR) underaction may arise from various causes that are distinguishable through imaging. We investigated clinical and imaging characteristics of congenital and acquired causes of IR underaction.
Methods: Cases of IR underaction were selected from data prospectively collected in a study of orbital imaging in strabismic patients.
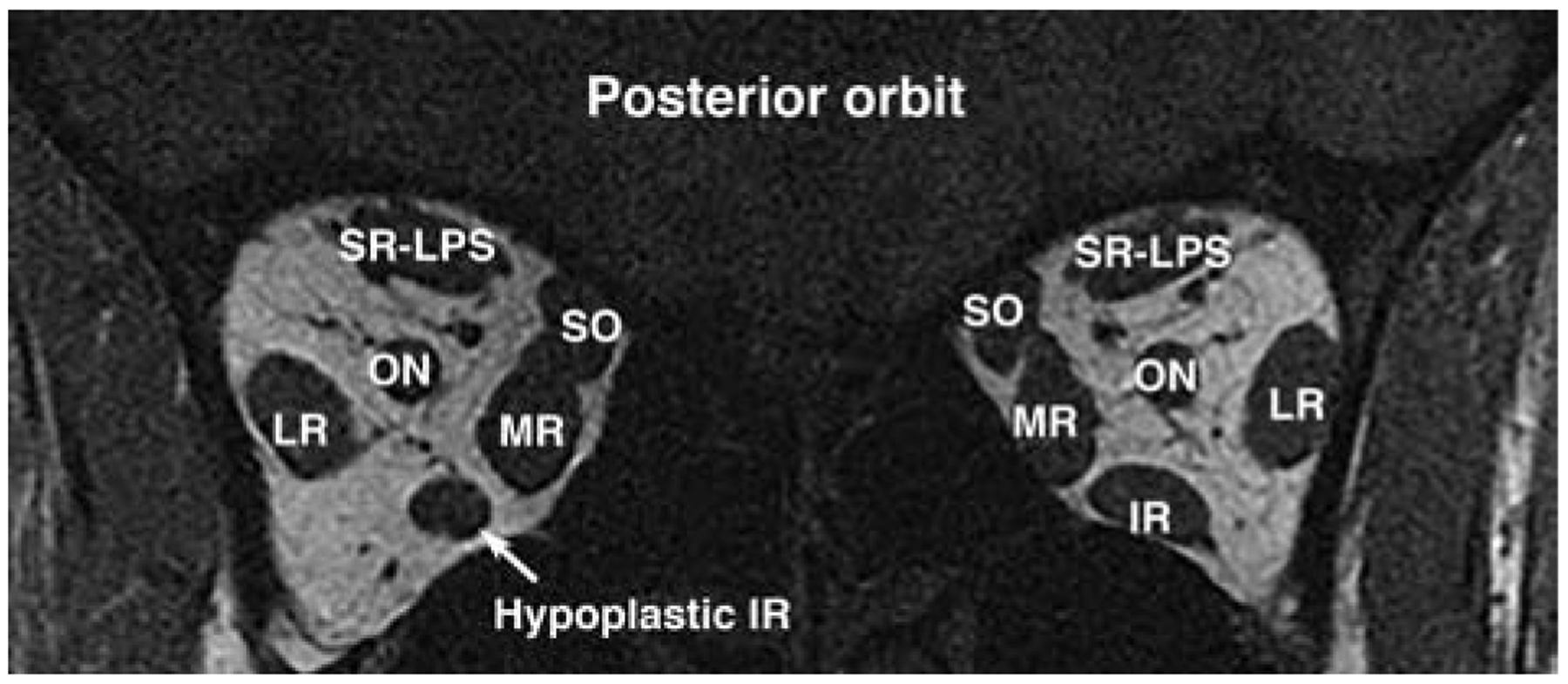
Results: Review identified 3 cases of congenital IR underaction (2 with bilateral IR aplasia and 1 with unilateral IR hypoplasia), 12 acquired cases, including 4 due to denervation (2 idiopathic, 1 after multiple strabismus surgeries, 1 after head trauma), and 8 cases of direct IR damage (5 with orbital trauma and 3 with previous surgery, including 2 sinus surgery and 1 laser blepharoplasty). Of the 23 cases, 11 adults had high-resolution magnetic resonance imaging, and 2 children had computed tomography. Imaging identified the anatomic diagnosis in congenital cases; in acquired cases, imaging helped to identify atrophy and exclude alternative orbital causes; and in direct mechanical damage, imaging clarified the mechanism of underaction, extent of IR damaged, and the degree of retained contractility. Patients with congenital IR absence or hypoplasia exhibited A pattern exotropia that was typically absent in isolated acquired denervation or direct IR damage.
Conclusions: Orbital imaging demonstrates a variety of abnormalities in patients with congenital or acquired IR hypofunction, helping to clarify the underlying mechanism and guide management.
Copyright © 2021 American Association for Pediatric Ophthalmology and Strabismus. Published by Elsevier Inc. All rights reserved.
Figures









References
-
- Chou TM, Demer JL. Isolated inferior rectus palsy caused by a metastasis to the oculomotor nucleus. Am J Ophthalmol 1998;126:737–40. - PubMed
-
- Akbari MR, Ameri A, Keshtkar Jaafari A, Fard MA, Eshraghi B, Mirmohammadsadeghi A. Clinical features and surgical outcomes of isolated inferior rectus muscle paralysis. Strabismus 2014;22:58–63. - PubMed
-
- Awadein A Clinical findings, orbital imaging, and intraoperative findings in patients with isolated inferior rectus muscle paresis or underaction. J AAPOS 2012;16:345–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
