

Targeting Cholesterol Metabolism as Efficient Antiviral Strategy Against the Hepatitis E Virus
- PMID: 33601063
- PMCID: PMC8099564
- DOI: 10.1016/j.jcmgh.2021.02.002
Targeting Cholesterol Metabolism as Efficient Antiviral Strategy Against the Hepatitis E Virus
Abstract
Background and aims: The Hepatitis E virus hijacks the endosomal system for its release. These structures are highly dependent on cholesterol. Hence, this study investigates the impact of HEV on cholesterol-metabolism, the effect of intracellular cholesterol content on HEV-release and the potential of cholesterol-modulators to serve as antivirals.
Methods: Intracellular cholesterol-content of cells was modulated and impacts on HEV were monitored using qPCR, Western blot, microscopy, virus-titration and density-gradient centrifugation. Blood-lipids and HEV-RNA were routinely quantified in chronically infected patients during follow-up visits.
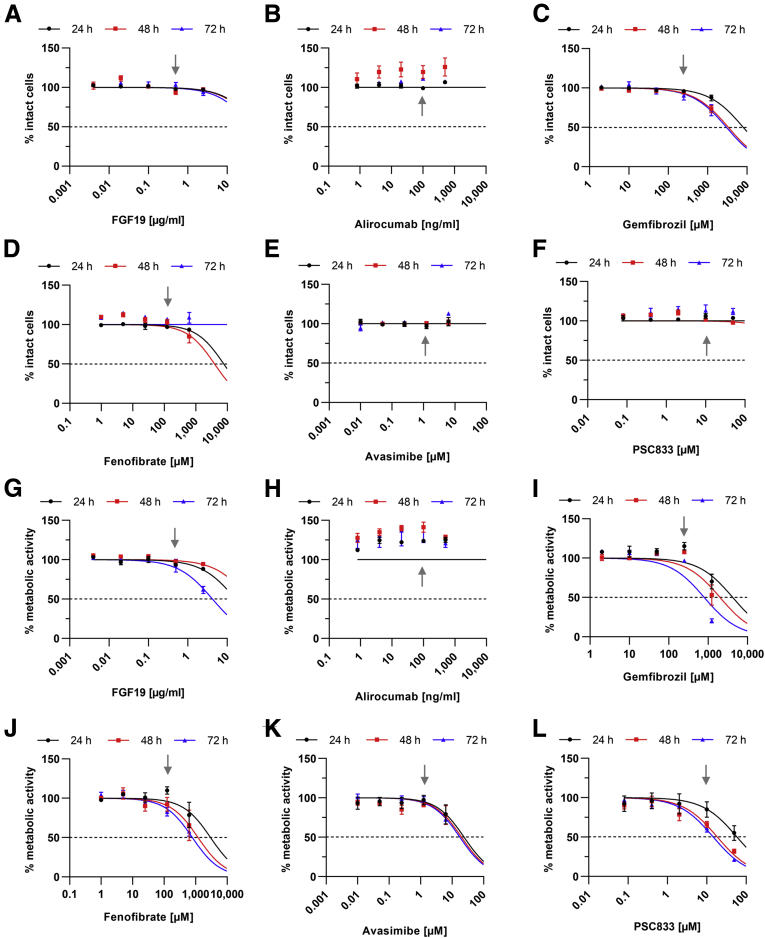
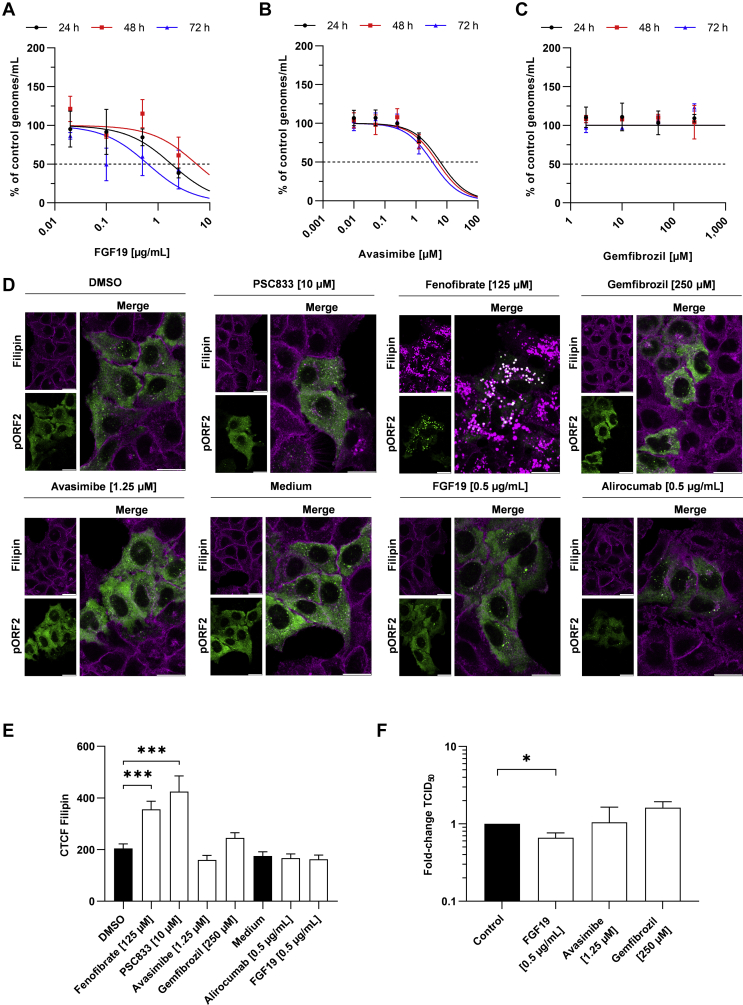
Results: In HEV-infected cells, decreased levels of cholesterol are found. In patients, HEV infection decreases serum-lipid concentrations. Importantly, statin treatment herein increases viral titers. Similarly, reduction of intracellular cholesterol via simvastatin treatment increases viral release in vitro. On the contrary, elevating intracellular cholesterol via LDL or 25-hydroxycholesterol strongly reduces viral release due to enhanced lysosomal degradation of HEV. Drug-induced elevation of intracellular cholesterol via fenofibrate or PSC833 impairs HEV release via the same mechanism.
Conclusions: This study analyses the crosstalk between HEV and intracellular cholesterol. The results highlight the importance of an intact cholesterol homeostasis for HEV-release and thereby identify a potential target for antiviral strategies. Especially fenofibrate is considered a promising novel antiviral against HEV. Beyond this, the study may help clinicians evaluating co-treatments of HEV-infected patients with statins, as this may be counter indicated.
Keywords: Antiviral; Cholesterol; HEV; Lipids; Lysosomes.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures












References
-
- Boxall E., Herborn A., Kochethu G., Pratt G., Adams D., Ijaz S., Teo C.-G. Transfusion-transmitted hepatitis E in a ‘nonhyperendemic’ country. Transfus Med. 2006;16:79–83. - PubMed
-
- Ricci A., Allende A., Bolton D., Chemaly M., Davies R., Fernandez Escamez P.S., Herman L., Koutsoumanis K., Lindqvist R., Nørrung B., Robertson L., Ru G., Sanaa M., Simmons M., Skandamis P., Snary E., Speybroeck N., Ter Kuile B., Threlfall J., Wahlström H., Di Bartolo I., Johne R., Pavio N., Rutjes S., van der Poel W., Vasickova P., Hempen M., Messens W., Rizzi V., Latronico F., Girone R. Public health risks associated with hepatitis E virus (HEV) as a food-borne pathogen. EFSA J. 2017;15:e4886. - PMC - PubMed
-
- Echevarría J.M., González J.E., Lewis-Ximenez L.L., Dos Santos D.R.L., Munné M.S., Pinto M.A., Pujol F.H., Rodríguez-Lay L.A. Hepatitis E virus infection in Latin America: a review. J Med Virol. 2013;85:1037–1045. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
