

Metabolic profiling reveals interleukin-17A monoclonal antibody treatment ameliorate lipids metabolism with the potentiality to reduce cardiovascular risk in psoriasis patients
- PMID: 33602246
- PMCID: PMC7890626
- DOI: 10.1186/s12944-021-01441-9
Metabolic profiling reveals interleukin-17A monoclonal antibody treatment ameliorate lipids metabolism with the potentiality to reduce cardiovascular risk in psoriasis patients
Abstract
Background: Psoriasis is a common chronic inflammatory skin disease associated with overproduction of interleukin-17A (IL-17A). IL-17A monoclonal antibodies (mAbs) have shown clinical efficacy in psoriasis patients. Although a series of different overlapping mechanisms have been found to establish a link between psoriasis and cardiovascular diseases, the underlying mechanisms of the two types of diseases and the potential efficacy of IL-17A mAbs in amelioration of cardiovascular comorbidities remain unclear.
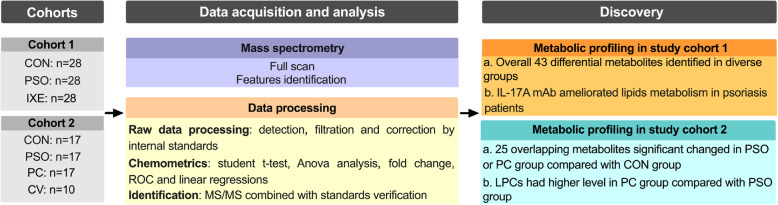
Methods: Serum samples from two study cohorts including 117 individuals were analyzed using a high-throughput UHPLC-MS platform. Non-targeted metabolic profiling analysis was first conducted with samples from 28 healthy individuals and from 28 psoriasis patients before and after 12-weeks of ixekizumab treatment in study cohort 1. Study cohort 2 was additionally recruited to validate the correlations of the identified metabolites with cardiovascular diseases.
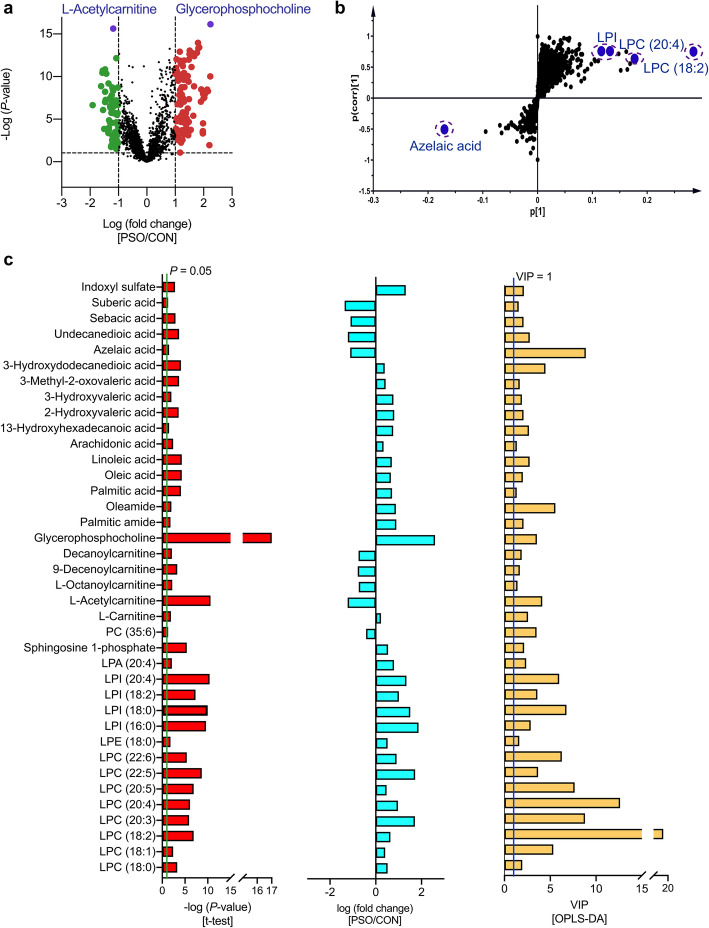
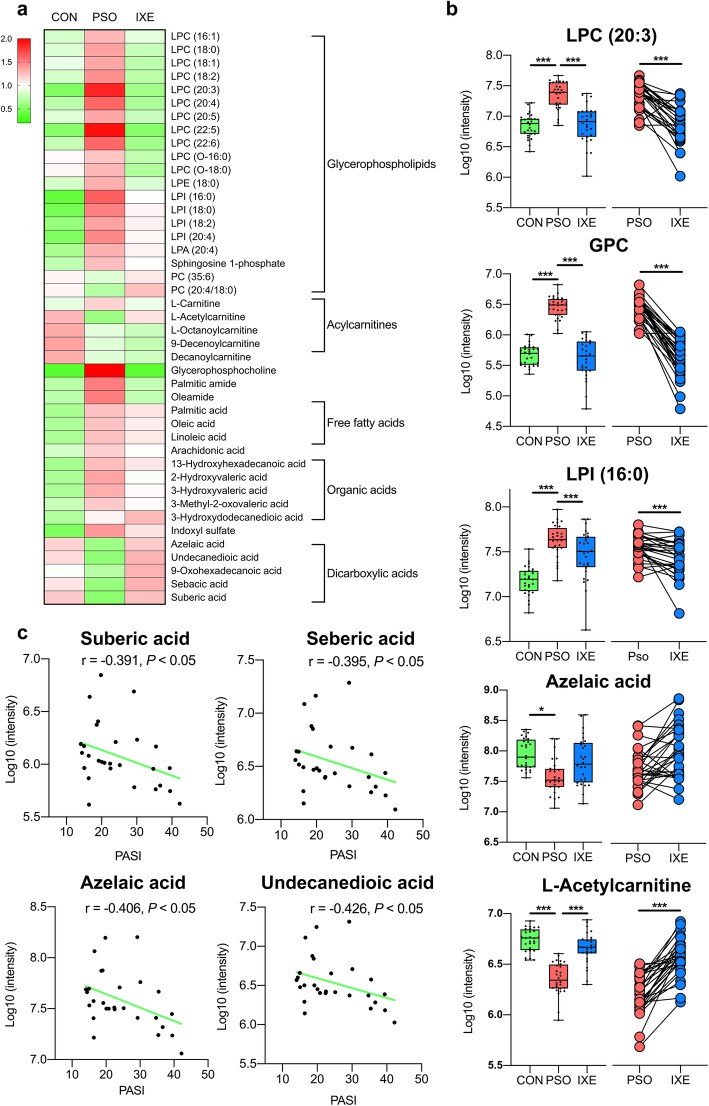
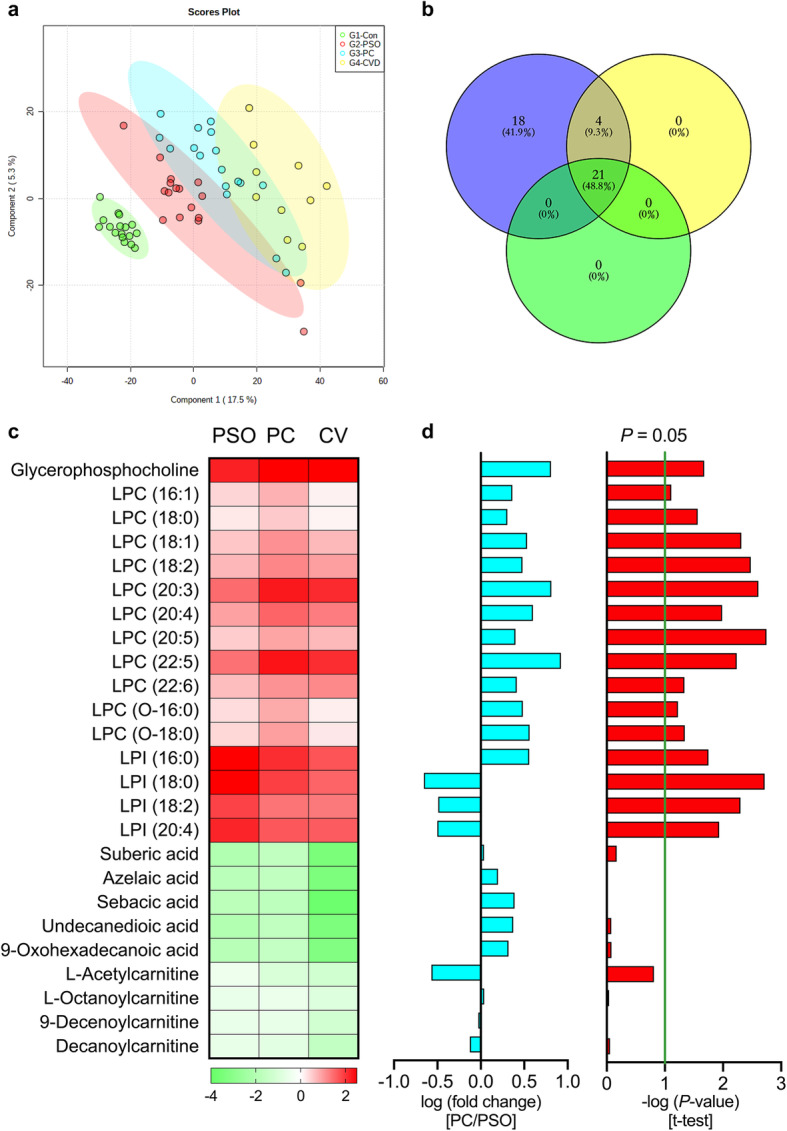
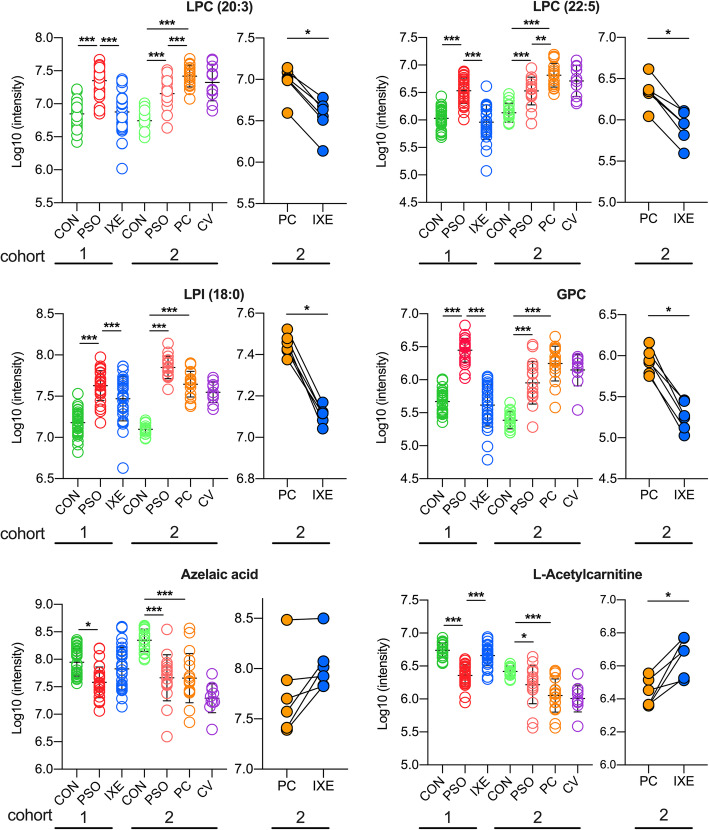
Results: A total of 43 differential metabolites, including lysophospholipids, free fatty acids, acylcarnitines and dicarboxylic acids, were accurately identified in study cohort 1, and the analysis showed that lipid metabolism was impaired in psoriasis patients. Compared with healthy individuals, psoriasis patients had higher levels of lysophosphatidylcholines, lysophosphatidylinositols, lysophosphatidic acids and free fatty acids, but lower levels of acylcarnitines and dicarboxylic acids. The identified dicarboxylic acid levels were inversely correlated with psoriasis area and severity index (PASI) scores (P < 0.05). The results for study cohort 2 were largely consistent with the results for study cohort 1. Moreover, the levels of all identified lysophosphatidylcholines were higher in psoriasis patients with coronary heart diseases than in psoriasis without coronary heart disease. Notably, most of these lipidic changes were ameliorated by ixekizumab treatment.
Conclusion: The results of this non-targeted metabolomic analysis indicate that treatment with IL-17A mAbs can not only ameliorate psoriasis lesions but also restore dysregulated lipid metabolism to normal levels in psoriasis patients. Considering that dysregulated lipid metabolism has been regarded as the critical factor in cardiovascular diseases, the recovery of lipid metabolites in psoriasis patients indicates that IL-17A mAbs might have the potential protective effects against cardiovascular comorbidities.
Keywords: Cardiovascular diseases; IL-17A monoclonal antibody; Ixekizumab; Lipids; Lysophospholipids; Metabolism; Psoriasis.
Conflict of interest statement
All authors declare that there are no conflicts of interest.
Figures
References
-
- Strauss H. Zur Lehre von der neurogenen und der thyreogenen Glykosurie. Dtsch Med Wochenschr. 1897;23:275e8.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
