

Platelets and lymphocytes drive progressive penumbral tissue loss during middle cerebral artery occlusion in mice
- PMID: 33602266
- PMCID: PMC7890632
- DOI: 10.1186/s12974-021-02095-1
Platelets and lymphocytes drive progressive penumbral tissue loss during middle cerebral artery occlusion in mice
Abstract
Background: In acute ischemic stroke, cessation of blood flow causes immediate tissue necrosis within the center of the ischemic brain region accompanied by functional failure in the surrounding brain tissue designated the penumbra. The penumbra can be salvaged by timely thrombolysis/thrombectomy, the only available acute stroke treatment to date, but is progressively destroyed by the expansion of infarction. The underlying mechanisms of progressive infarction are not fully understood.
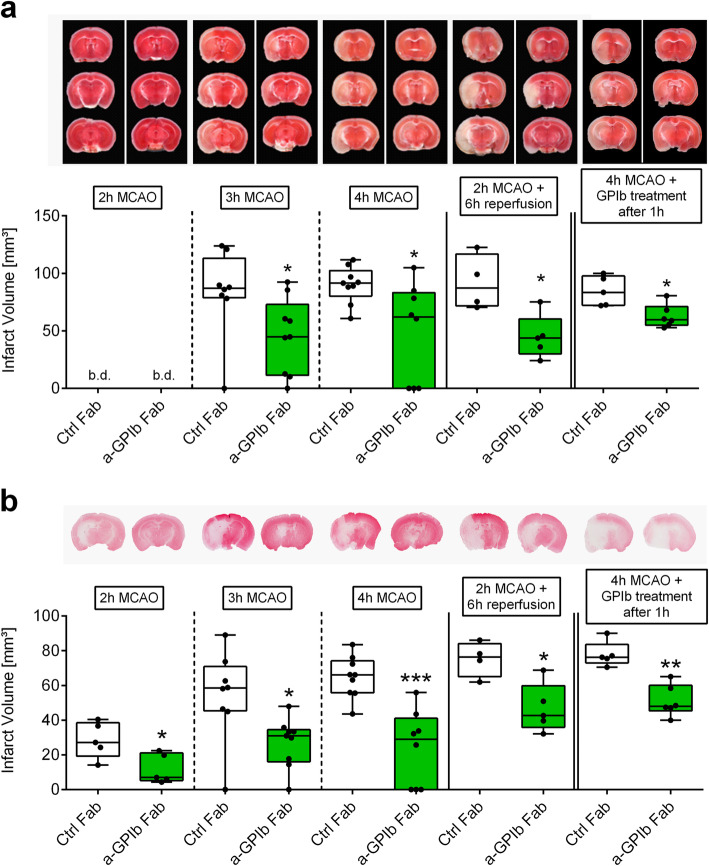
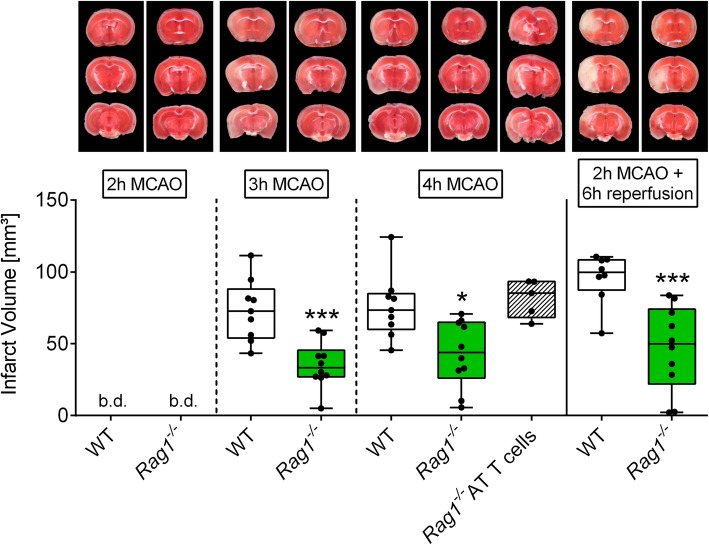
Methods: To address mechanisms, mice underwent filament occlusion of the middle cerebral artery (MCAO) for up to 4 h. Infarct development was compared between mice treated with antigen-binding fragments (Fab) against the platelet surface molecules GPIb (p0p/B Fab) or rat immunoglobulin G (IgG) Fab as control treatment. Moreover, Rag1-/- mice lacking T-cells underwent the same procedures. Infarct volumes as well as the local inflammatory response were determined during vessel occlusion.
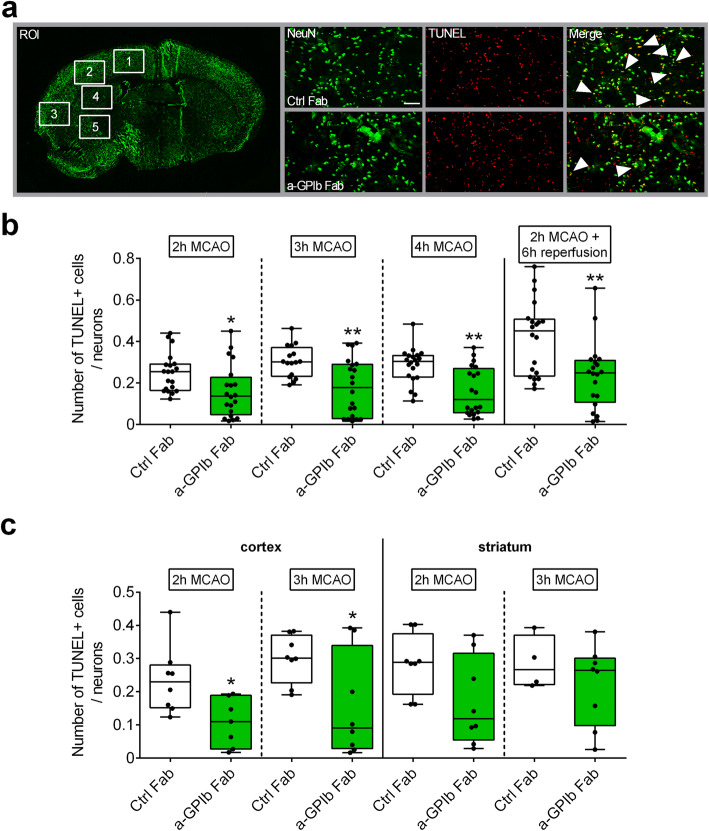
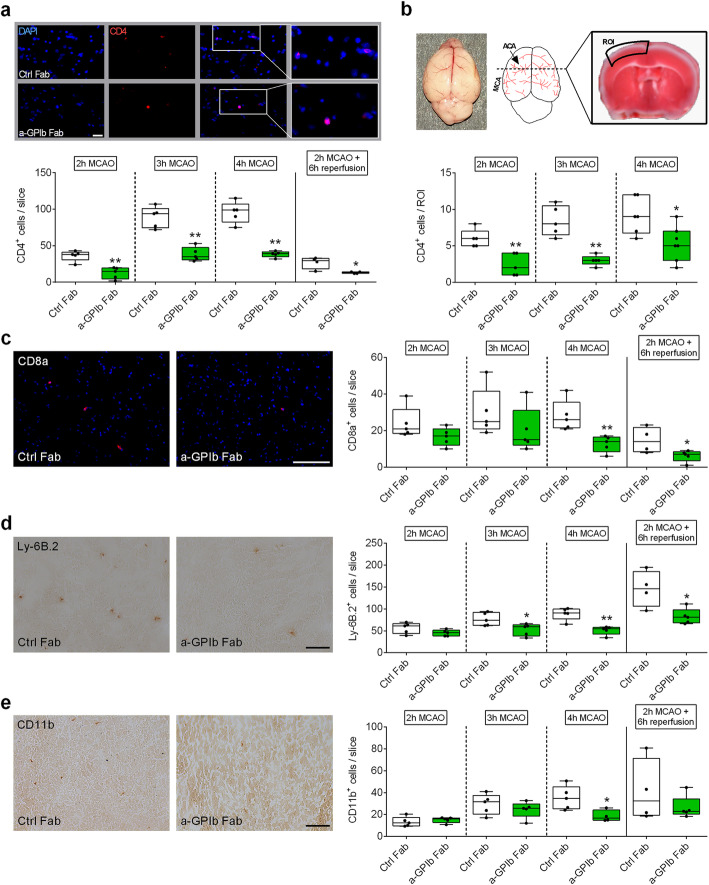
Results: We show that blocking of the platelet adhesion receptor, glycoprotein (GP) Ibα in mice, delays cerebral infarct progression already during occlusion and thus before recanalization/reperfusion. This therapeutic effect was accompanied by decreased T-cell infiltration, particularly at the infarct border zone, which during occlusion is supplied by collateral blood flow. Accordingly, mice lacking T-cells were likewise protected from infarct progression under occlusion.
Conclusions: Progressive brain infarction can be delayed by blocking detrimental lymphocyte/platelet responses already during occlusion paving the way for ultra-early treatment strategies in hyper-acute stroke before recanalization.
Keywords: Glycoprotein receptor Ib; Ischemic penumbra; Ischemic stroke; T-cells; Thrombo-inflammation; middle cerebral artery occlusion.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, Davalos A, Majoie CB, van der Lugt A, de Miquel MA, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387:1723–1731. doi: 10.1016/S0140-6736(16)00163-X. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
