

Comparing Patterns of Care for Febrile Infants at Community and University-Affiliated Hospitals
- PMID: 33602793
- PMCID: PMC7898233
- DOI: 10.1542/hpeds.2020-000778
Comparing Patterns of Care for Febrile Infants at Community and University-Affiliated Hospitals
Abstract
Objectives: Most children in the United States receive treatment in community hospitals, but descriptions of clinical practice patterns in pediatric care in this setting are lacking. Our objectives were to compare clinical practice patterns primarily between community and university-affiliated hospitals and secondarily by number of pediatric beds before and during participation in a national practice standardization project.
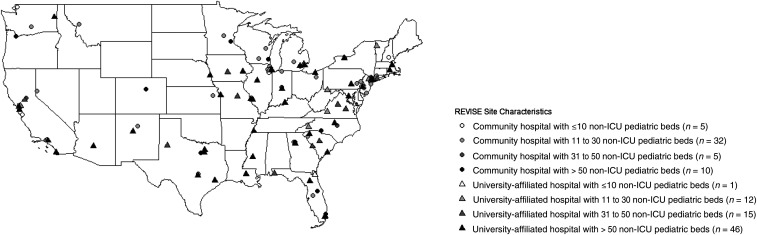
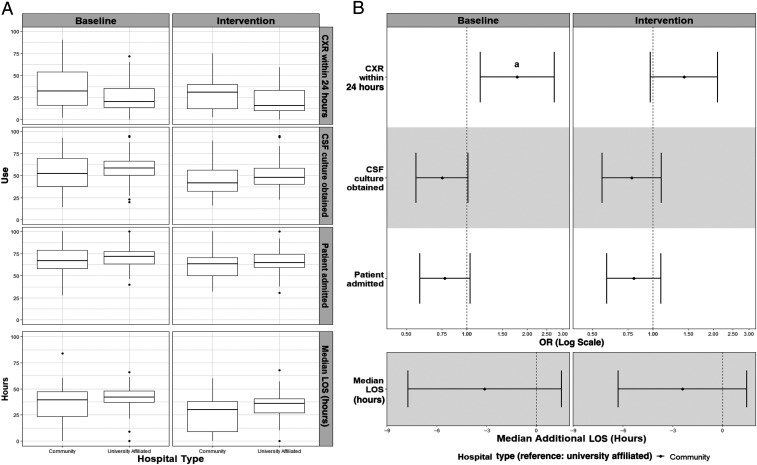
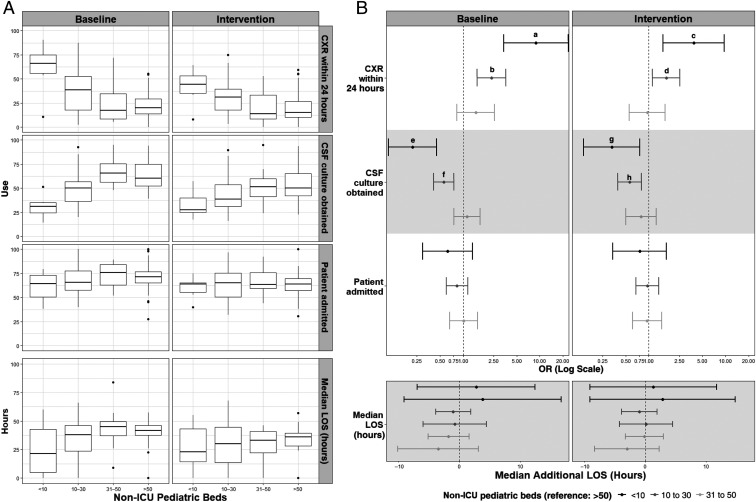
Methods: We performed a retrospective secondary analysis on data from 126 hospitals that participated in the American Academy of Pediatrics' Value in Inpatient Pediatrics Reducing Excessive Variability in the Infant Sepsis Evaluation project, a national quality improvement project conducted to improve care for well-appearing febrile infants aged 7 to 60 days. Four use measures were compared by hospital type and by number of non-ICU pediatric beds.
Results: There were no differences between community and university-affiliated hospitals in the odds of hospital admission, average length of stay, or odds of cerebrospinal fluid culture. The odds of chest radiograph at community hospitals were higher only during the baseline period. There were no differences by number of pediatric beds in odds of admission or average length of stay. For hospitals with ≤30 pediatric beds, the odds of chest radiograph were higher and the odds of cerebrospinal fluid culture were lower compared with hospitals >50 beds during both study periods.
Conclusions: In many key aspects, care for febrile infants does not differ between community and university-affiliated hospitals. Clinical practice may differ more by number of pediatric beds.
Copyright © 2021 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: Dr Biondi provides consultation for McKesson Incorporated; the other authors have indicated they have no potential conflicts of interest to disclose.
Figures
References
-
- McDaniel CE, Jennings R, Schroeder AR, Paciorkowski N, Hofmann M, Leyenaar J. Aligning inpatient pediatric research with settings of care: a call to action. Pediatrics. 2019;143(5):e20182648. - PubMed
-
- Keren R, Luan X, Localio R, et al. ; Pediatric Research in Inpatient Settings (PRIS) Network. Prioritization of comparative effectiveness research topics in hospital pediatrics. Arch Pediatr Adolesc Med. 2012;166(12):1155–1164 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
