

Fecal microbiota transplantation in HIV: A pilot placebo-controlled study
- PMID: 33602945
- PMCID: PMC7892558
- DOI: 10.1038/s41467-021-21472-1
Fecal microbiota transplantation in HIV: A pilot placebo-controlled study
Abstract
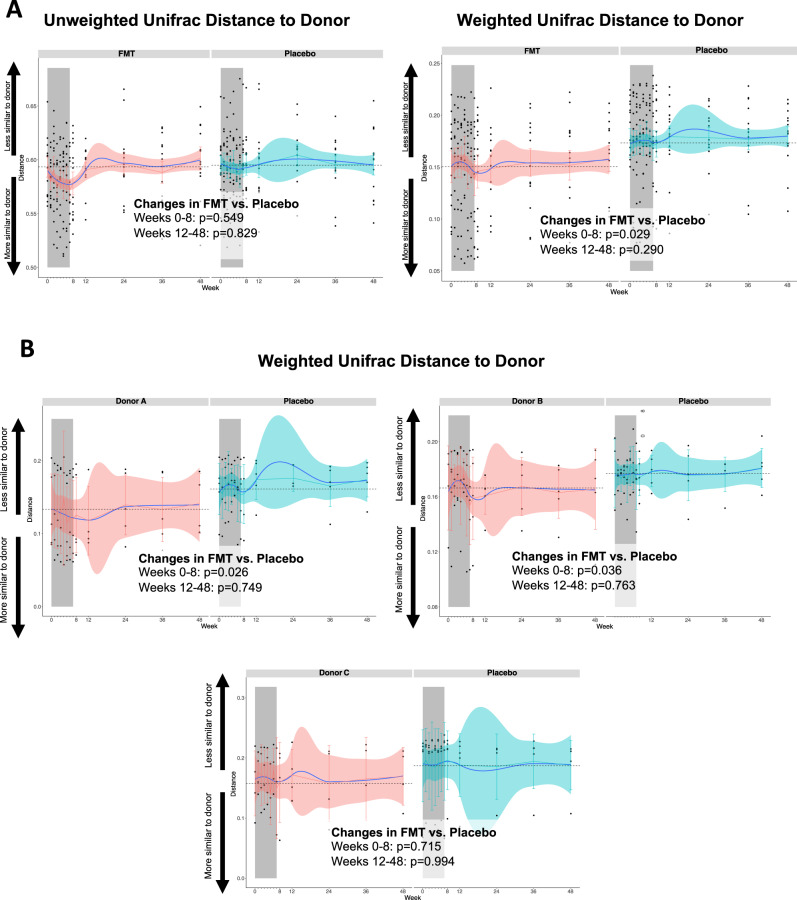
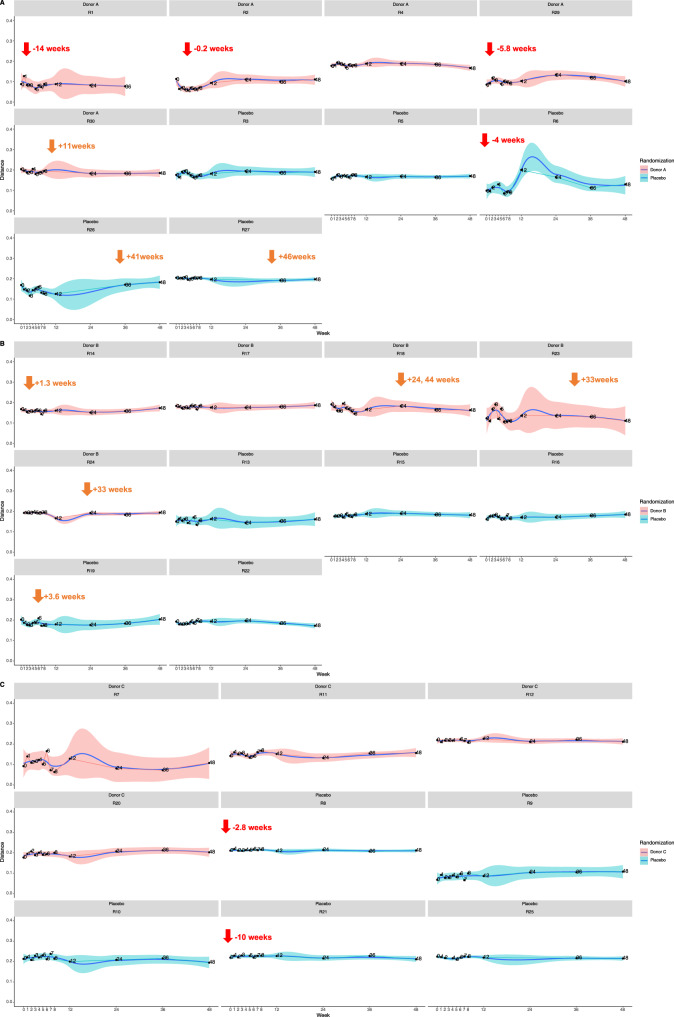
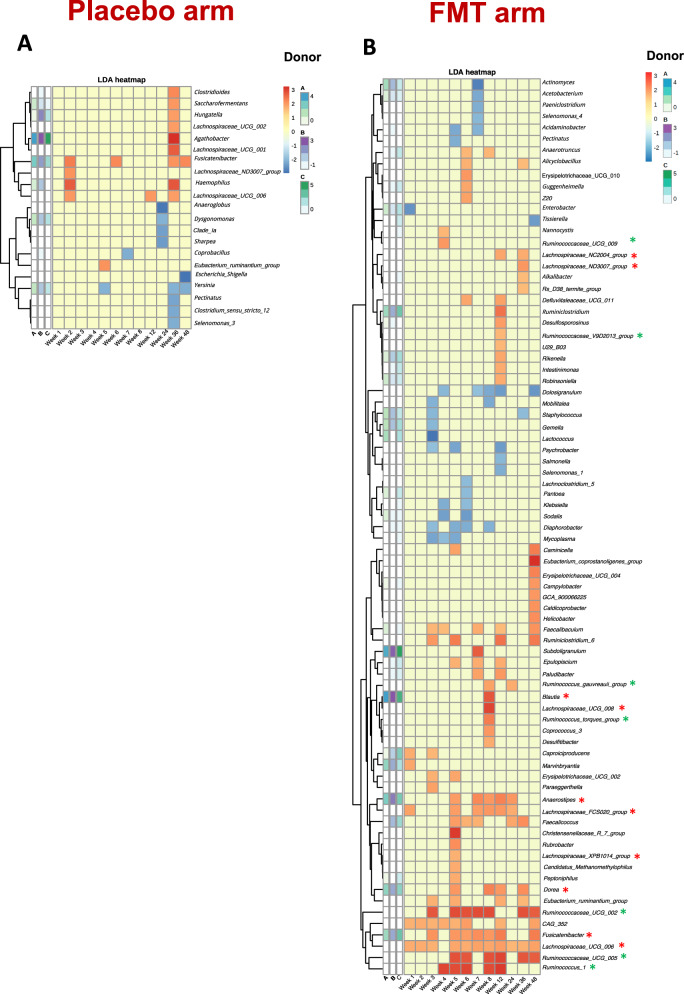
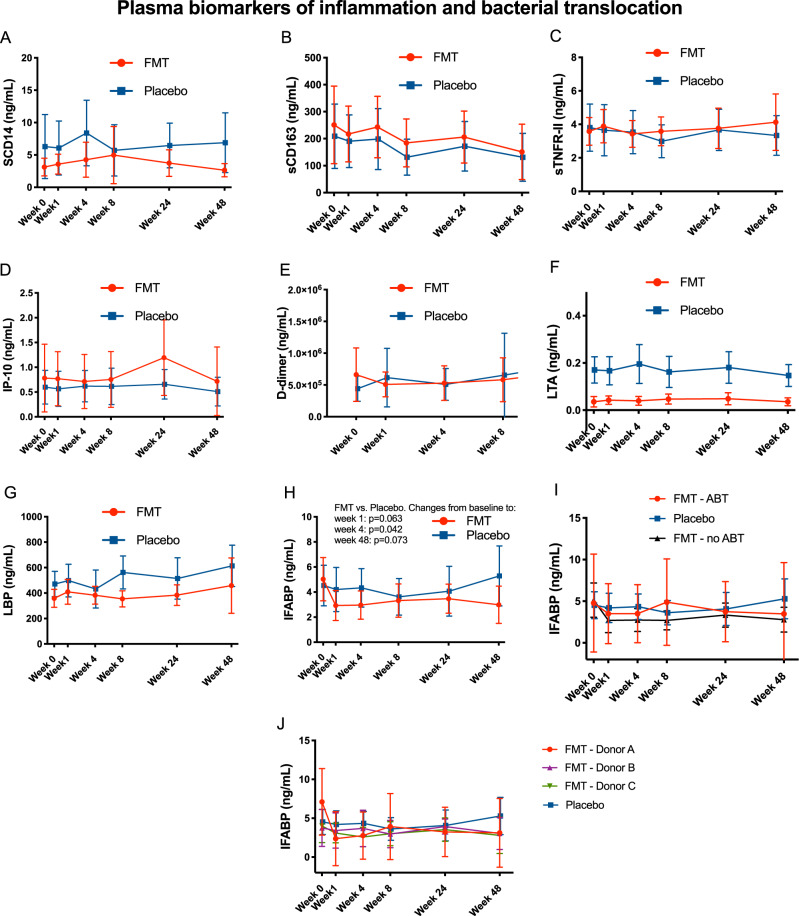
Changes in the microbiota have been linked to persistent inflammation during treated HIV infection. In this pilot double-blind study, we study 30 HIV-infected subjects on antiretroviral therapy (ART) with a CD4/CD8 ratio < 1 randomized to either weekly fecal microbiota capsules or placebo for 8 weeks. Stool donors were rationally selected based on their microbiota signatures. We report that fecal microbiota transplantation (FMT) is safe, not related to severe adverse events, and attenuates HIV-associated dysbiosis. FMT elicits changes in gut microbiota structure, including significant increases in alpha diversity, and a mild and transient engraftment of donor's microbiota during the treatment period. The greater engraftment seems to be achieved by recent antibiotic use before FMT. The Lachnospiraceae and Ruminococcaceae families, which are typically depleted in people with HIV, are the taxa more robustly engrafted across time-points. In exploratory analyses, we describe a significant amelioration in the FMT group in intestinal fatty acid-binding protein (IFABP), a biomarker of intestinal damage that independently predicts mortality. Gut microbiota manipulation using a non-invasive and safe strategy of FMT delivery is feasible and deserves further investigation. Trial number: NCT03008941.
Conflict of interest statement
Outside the submitted work, S.S.-V. reports personal fees from ViiV Healthcare, Janssen Cilag, Gilead Sciences, and MSD as well as non-financial support from ViiV Healthcare and Gilead Sciences and research grants from MSD and Gilead Sciences. J.M.-S. reports non-financial support from ViiV Healthcare, Gilead Sciences, and Jannsen Cilag. J.P. reports grants, personal fees and non-financial support from ViiV Healthcare; grants, personal fees, and non-financial support from Gilead Sciences; grants, personal fees, and non-financial support from Janssen Cilag; personal fees from MSD; and personal fees from Abbvie. F.D. reports personal fees from Gilead. J.M.S. reports personal fees from ViiV Healthcare, Janssen Cilag, and Gilead Sciences. MJ.V. reports personal fees from Gilead Sciences, non-financial support from ViiV Healthcare, and Gilead Sciences, and grants from ViiV Healthcare. S.M. reports personal fees and non-financial from ViiV Healthcare, Janssen, Gilead Sciences, and MSD, as well as grants from MSD, ViiV Healthcare, and Gilead Sciences. S.B. and M.O. work for OpenBiome. R.E. was an employee at OpenBiome during the conduct of this study. A.T.-R., M.J.G., N.M., B.N., V.L., A.V., J.Z., C.G., M.M., R.R., S.H., U.A., and A.M. report no conflicts of interest.
Figures


References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
