

Rotational Changes in the Distal Tibial Fragment Relative to the Proximal Tibial Fragment at the Osteotomy Site after Open-Wedge High-Tibial Osteotomy
- PMID: 33604377
- PMCID: PMC7870301
- DOI: 10.1155/2021/6357109
Rotational Changes in the Distal Tibial Fragment Relative to the Proximal Tibial Fragment at the Osteotomy Site after Open-Wedge High-Tibial Osteotomy
Abstract
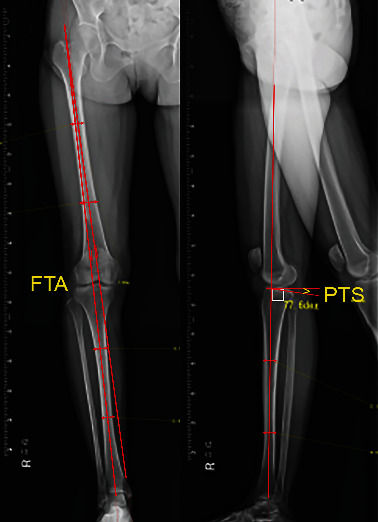
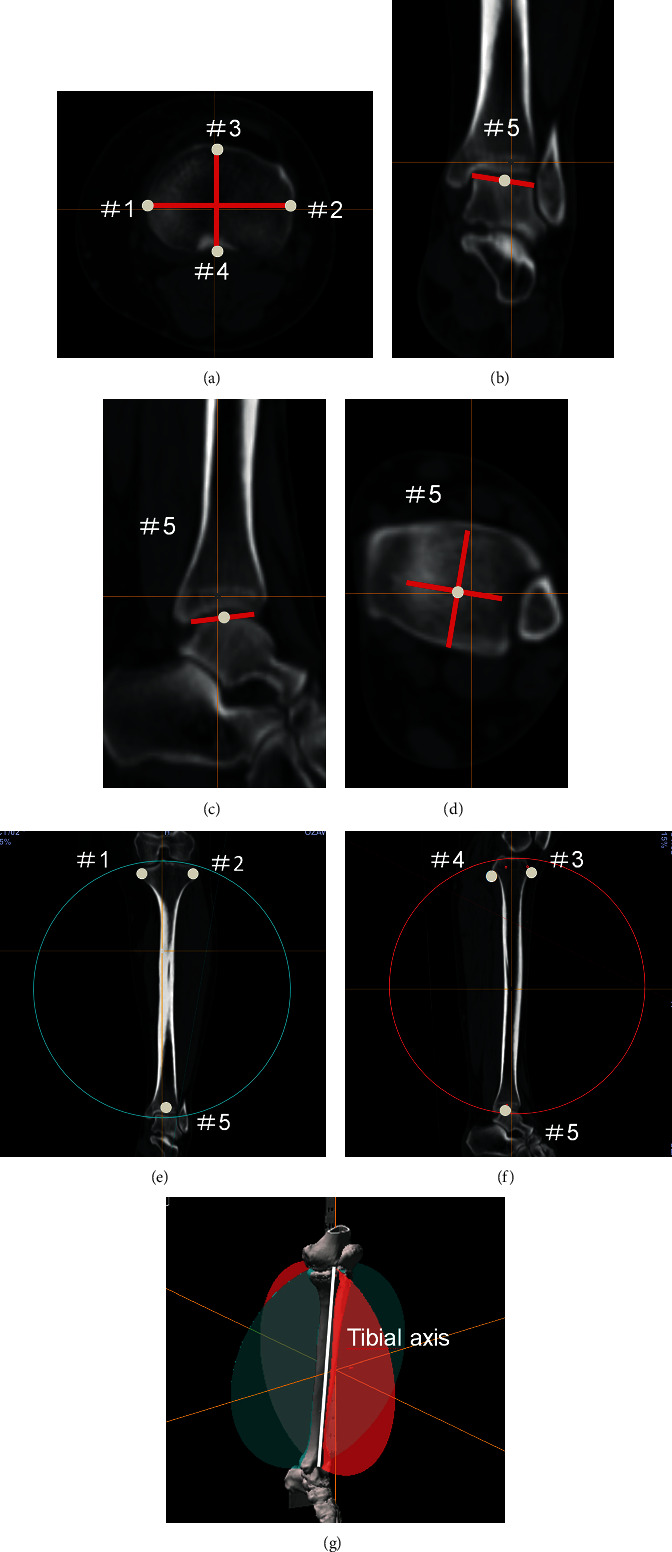
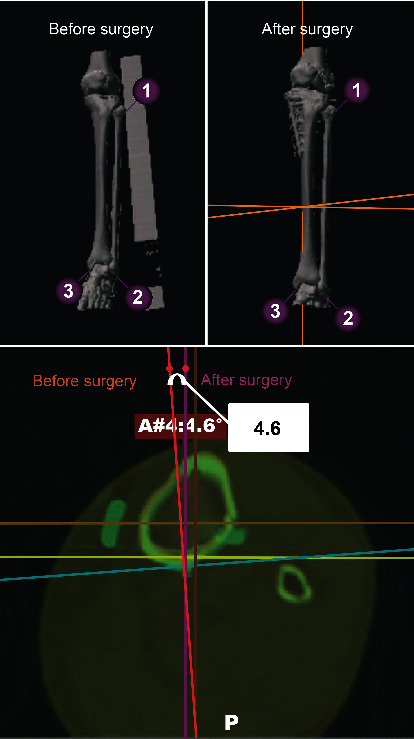
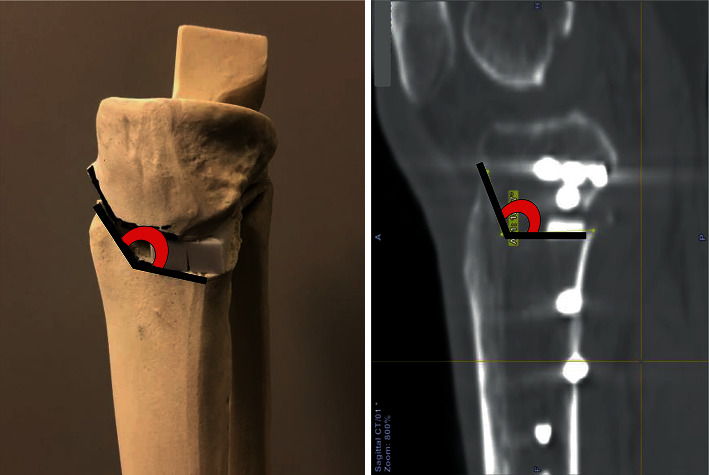
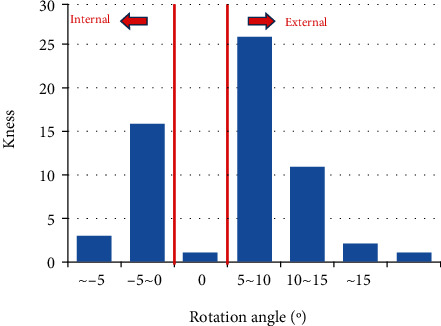
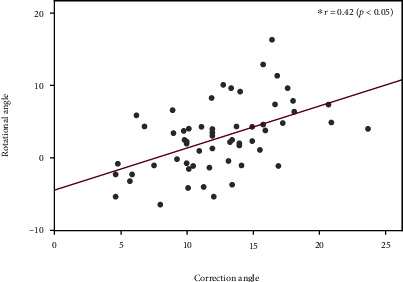
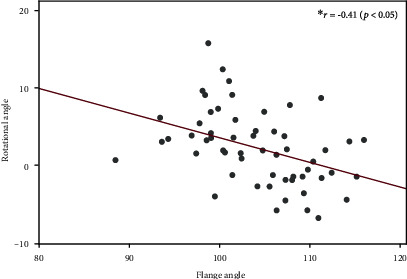
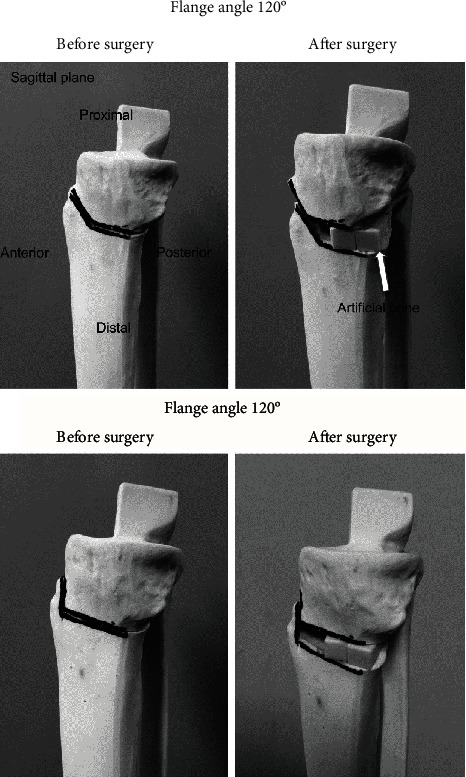
The present study is aimed at assessing the changes in tibial rotation at the osteotomy site after an open-wedge, high-tibial osteotomy (OWHTO) and analysing the factors that affect rotational changes in the distal tibial fragment relative to the proximal tibial fragment at the same site. This study involved 53 patients (60 knees; 16 males and 37 females) with medial osteoarthritis (OA) who underwent OWHTO and preoperative and 3-month postoperative computed tomography (CT) scans. Rotational angles of the distal tibia were measured using Stryker OrthoMap 3D by comparing preoperative and postoperative CTs. The mean rotational angle yielded an external rotation of 2.9° ± 4.8°. There were 17 knees with internal rotations, 37 knees with external rotations, and one knee with no rotation. The rotational angle significantly correlated with the resultant change in the femorotibial angle (correction angle) and the angle between the ascending and transverse osteotomy lines on the anterior osteotomised surface on which a flange was formed with the distal tibial osteotomised surface (flange angle). The flange angle affected the rotation, but it may have been affected by our surgical technique. The rotational angle did not significantly correlate with the change in the angle of the posterior tibial slope or body mass index. There were significant correlations between the rotational angle and correction angle (r = 0.42, p < 0.05). Additionally, the rotational angle correlated with the flange angle (r = -0.41, p < 0.05).
Copyright © 2021 Takahiro Sasaki et al.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this paper.
Figures
Similar articles
-
Comparison of torsional changes in the tibia following a lateral closed or medial open wedge high tibial osteotomy.Knee. 2019 Mar;26(2):374-381. doi: 10.1016/j.knee.2019.01.009. Epub 2019 Feb 14. Knee. 2019. PMID: 30772185
-
Three-dimensional relationships between secondary changes and selective osteotomy parameters for biplane medial open-wedge high tibial osteotomy.Knee. 2017 Mar;24(2):362-371. doi: 10.1016/j.knee.2016.11.010. Epub 2017 Feb 4. Knee. 2017. PMID: 28169100
-
Unintended Rotational Changes of the Distal Tibia After Biplane Medial Open-Wedge High Tibial Osteotomy.J Arthroplasty. 2016 Jan;31(1):59-63. doi: 10.1016/j.arth.2015.08.010. Epub 2015 Aug 14. J Arthroplasty. 2016. PMID: 26387921
-
Rotational Changes in the Tibia After High Tibial Valgus Osteotomy: A Comparative Study of Lateral Closing Versus Medial Opening Wedge Osteotomy.Am J Sports Med. 2020 Dec;48(14):3549-3556. doi: 10.1177/0363546520960114. Epub 2020 Oct 22. Am J Sports Med. 2020. PMID: 33090892
-
Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy.Arthroscopy. 2004 Apr;20(4):366-72. doi: 10.1016/j.arthro.2004.01.024. Arthroscopy. 2004. PMID: 15067275 Review.
Cited by
-
Hybrid Closed Wedge High Tibial Osteotomy Maintains the Leg Length After Surgery Compared With Open Wedge High Tibial Osteotomy.Cureus. 2024 Apr 10;16(4):e57953. doi: 10.7759/cureus.57953. eCollection 2024 Apr. Cureus. 2024. PMID: 38738055 Free PMC article.
-
Can double-level osteotomy prevent patellofemoral osteoarthritis progression compared with open wedge high tibial osteotomy?Arch Orthop Trauma Surg. 2023 Apr;143(4):2073-2085. doi: 10.1007/s00402-022-04523-0. Epub 2022 Jul 9. Arch Orthop Trauma Surg. 2023. PMID: 35809099
-
Effects of different hinge positions on tibial rotation in uniplanar medial opening wedge high tibial osteotomy with three-dimensional tibial models.Front Surg. 2024 Oct 30;11:1441777. doi: 10.3389/fsurg.2024.1441777. eCollection 2024. Front Surg. 2024. PMID: 39539509 Free PMC article.
-
Osseous factors influencing distal tibial rotation in biplane medial opening wedge high tibial osteotomy.Int Orthop. 2024 Feb;48(2):465-471. doi: 10.1007/s00264-023-05968-7. Epub 2023 Sep 14. Int Orthop. 2024. PMID: 37707599
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
