

Characteristics and Outcome of SARS-CoV-2 Infection in Cancer Patients
- PMID: 33604509
- PMCID: PMC7665636
- DOI: 10.1093/jncics/pkaa090
Characteristics and Outcome of SARS-CoV-2 Infection in Cancer Patients
Abstract
Background: Concerns have emerged about the higher risk of fatal coronavirus disease 2019 (COVID-19) in cancer patients. In this article, we review the experience of a comprehensive cancer center.
Methods: A prospective registry was set up at Institut Curie at the beginning of the COVID-19 pandemic. All cancer patients with suspected or proven COVID-19 were entered and actively followed for 28 days.
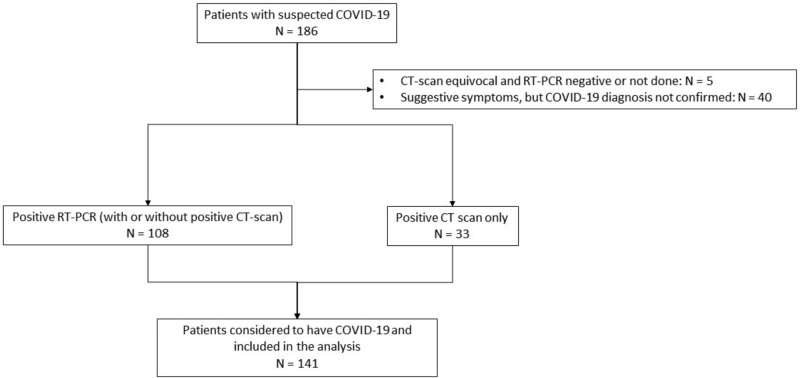
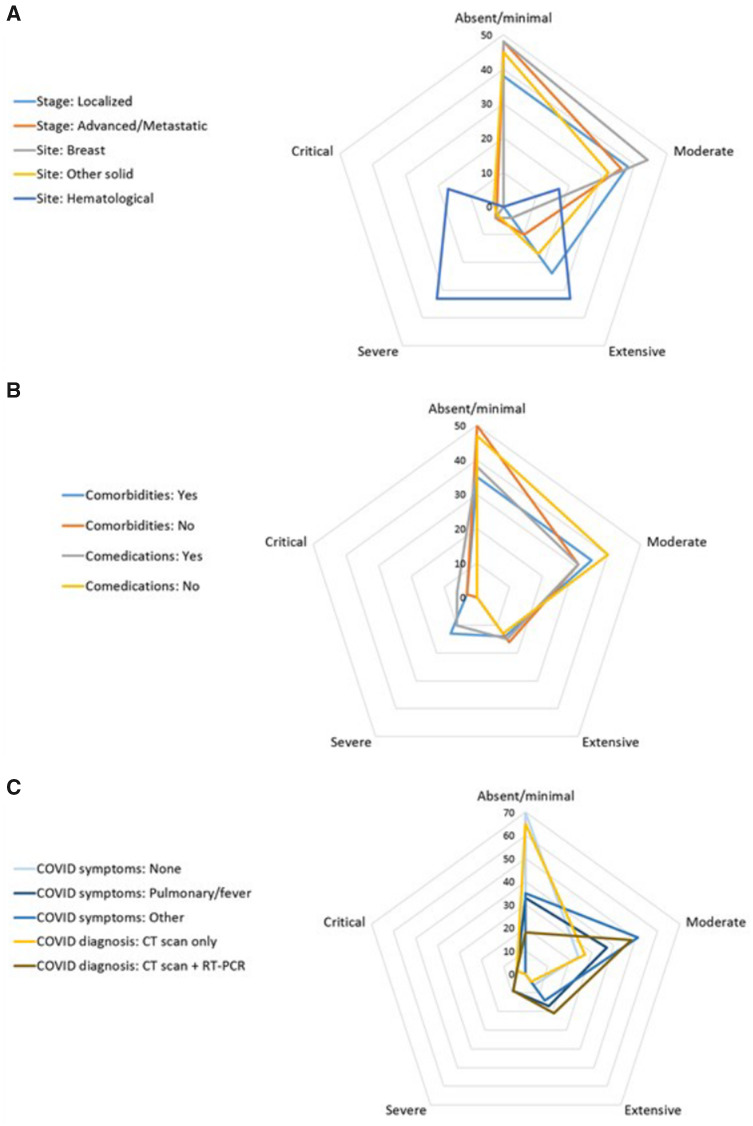
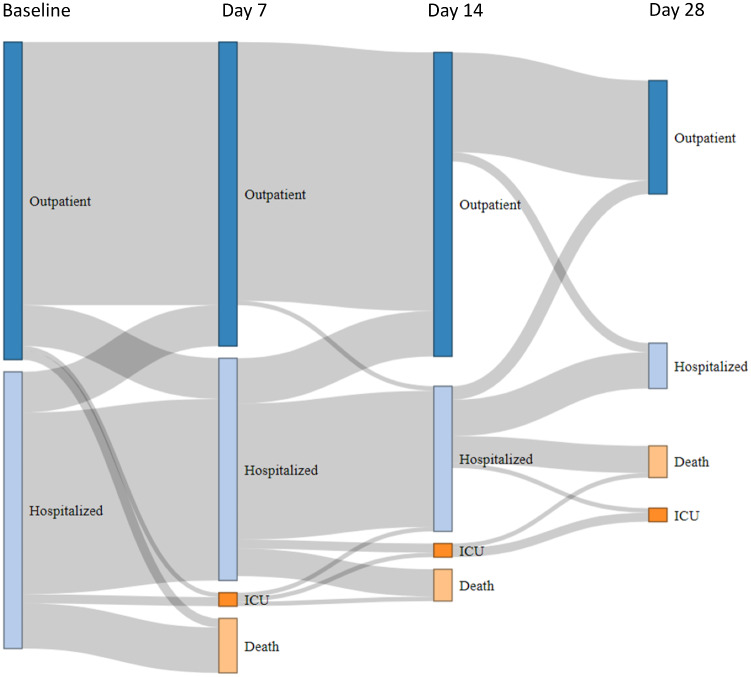
Results: Among 9842 patients treated at Institut Curie between March 13 and May 1, 2020, 141 (1.4%) were diagnosed with COVID-19, based on reverse transcription polymerase chain reaction testing and/or computerized tomography scan. In line with our case mix, breast cancer (40.4%) was the most common tumor type, followed by hematological and lung malignancies. Patients with active cancer therapy or/and advanced cancer accounted for 87.9% and 68.9% of patients, respectively. At diagnosis, 78.7% of patients had COVID-19-related symptoms, with an extent of lung parenchyma involvement inferior to 50% in 95.8% of patients. Blood count variations and C-reactive protein elevation were the most common laboratory abnormalities. Antibiotics and antiviral agents were administered in 48.2% and 6.4% of patients, respectively. At the time of analysis, 26 patients (18.4%) have died from COVID-19, and 100 (70.9%) were cured. Independent prognostic factors at the time of COVID-19 diagnosis associated with death or intensive care unit admission were extent of COVID-19 pneumonia and decreased O2 saturation.
Conclusions: COVID-19 incidence and presentation in cancer patients appear to be very similar to those in the general population. The outcome of COVID-19 is primarily driven by the initial severity of infection rather than patient or cancer characteristics.
© The Author(s) 2021. Published by Oxford University Press.
Figures
References
-
- World Health Organization. Coronavirus Disease outbreak news. https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/. Accessed July 10, 2020.
-
- Johns Hopkins coronavirus dashboard. https://coronavirus.jhu.edu/map.html. Accessed July 10, 2020.
-
- Informations Corononavirus. https://www.gouvernement.fr/info-coronavirus. Accessed July 10, 2020.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous