

Dialysis Initiation and All-Cause Mortality Among Incident Adult Patients With Advanced CKD: A Meta-analysis With Bias Analysis
- PMID: 33604540
- PMCID: PMC7873831
- DOI: 10.1016/j.xkme.2020.09.013
Dialysis Initiation and All-Cause Mortality Among Incident Adult Patients With Advanced CKD: A Meta-analysis With Bias Analysis
Abstract
Rationale & objectives: Due to unmeasured confounding, observational studies have limitations when assessing whether dialysis initiation reduces mortality compared with conservative therapy among adults with advanced chronic kidney disease (CKD). We addressed this issue in this meta-analysis.
Study design: Meta-analysis with bias analysis for unmeasured confounding.
Setting & study population: Adults with stage 4 or 5 CKD who had initiated dialysis or conservative treatment.
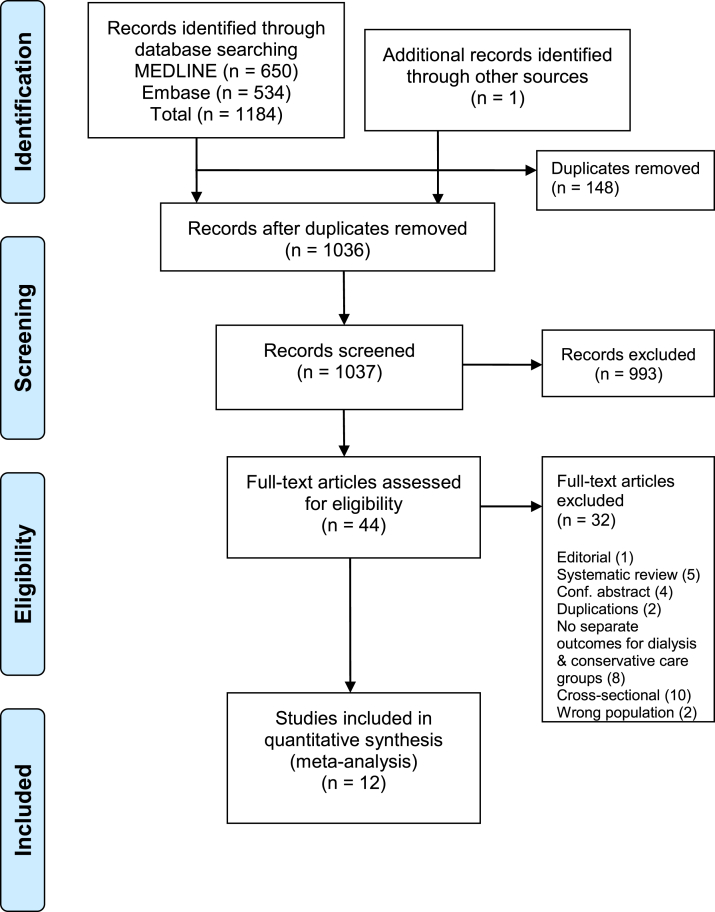
Selection criteria for studies: Prospective or retrospective cohort studies comparing survival of dialysis versus conservatively managed patients were searched on MEDLINE and Embase from January 2009 to March 20, 2019.
Data extraction: HRs of all-cause mortality associated with dialysis initiation compared with conservative treatment.
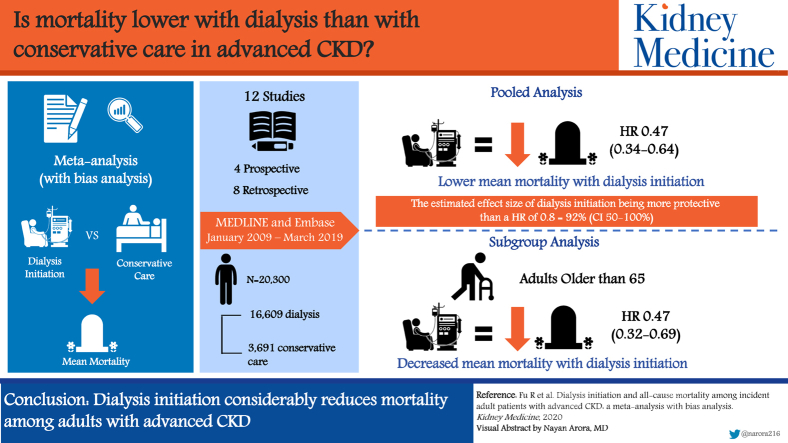
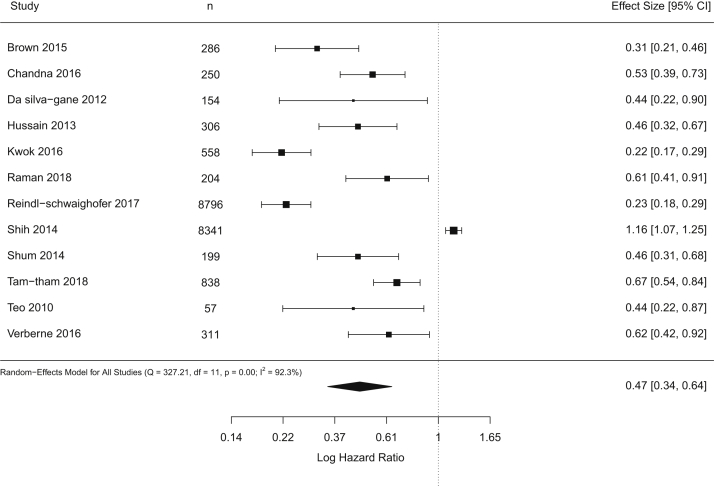
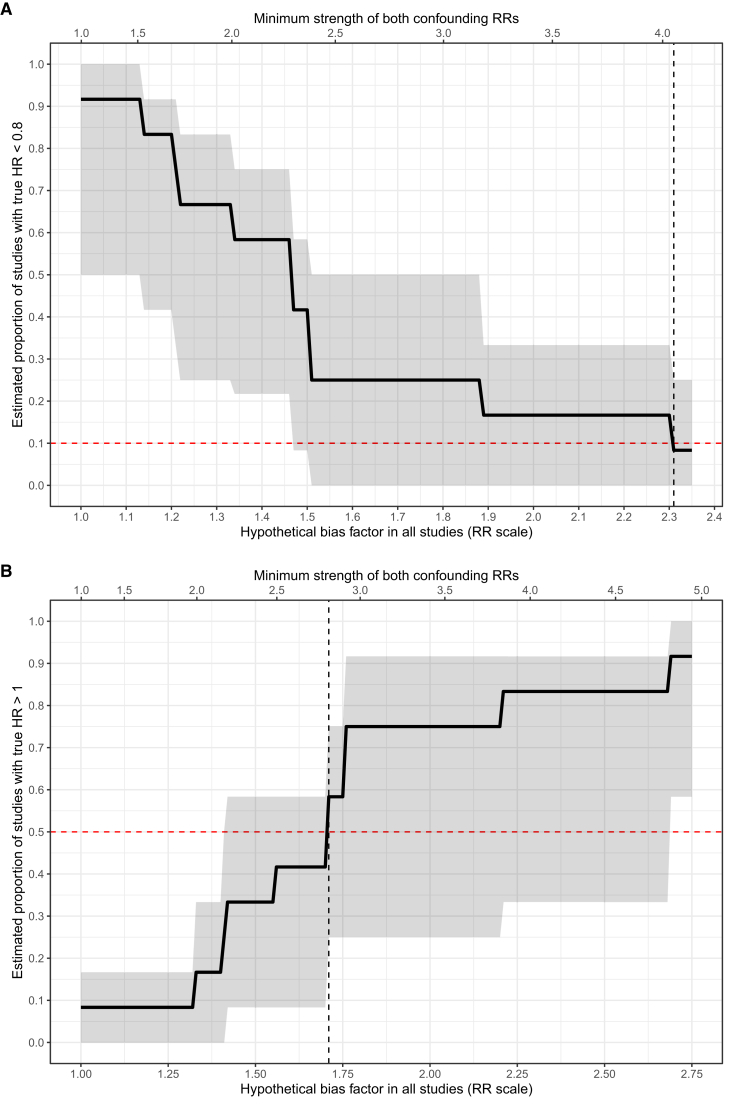
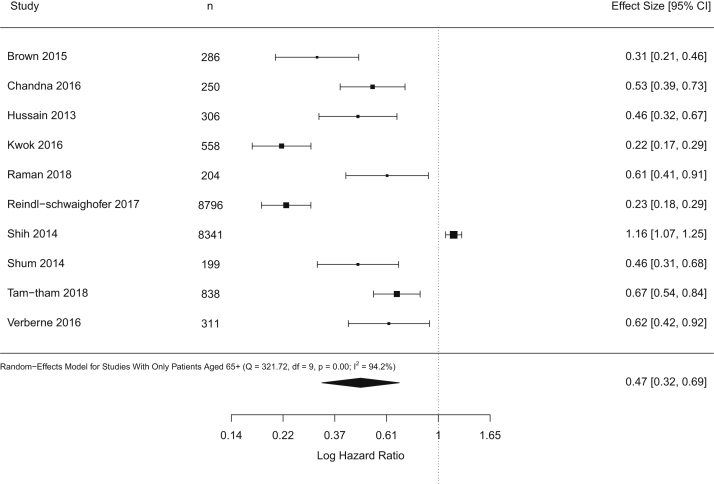
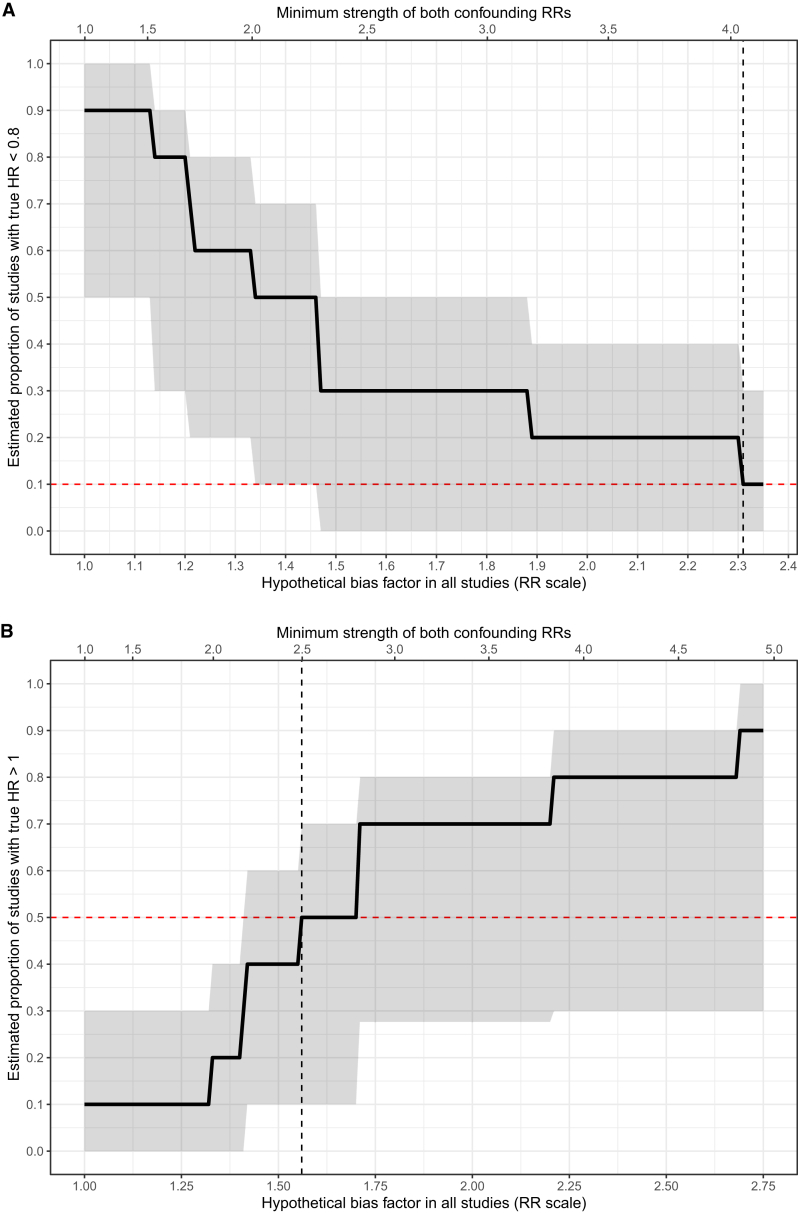
Analytical approach: We pooled HRs using a random-effects model. We estimated the percentage of effect sizes more protective than HRs of 0.80 and severity of unmeasured confounding that could reduce this percentage to only 10%. Subgroup analysis was performed for studies with only older patients (aged ≥ 65 years).
Results: 12 studies were included that involved 16,609 dialysis patients and 3,691 conservatively managed patients. A random-effects model suggested that dialysis initiation was associated with a mean mortality HR of 0.47 (95% CI, 0.34-0.64), in which 92% (95% CI, 50%-100%) of the true effects were more protective than HRs of 0.80. To reduce the percentage of HRs < 0.80 to 10%, unmeasured confounder(s) would need to be associated with both dialysis initiation and mortality by relative risks of 4.05 (95% CI, 2.39-4.15), which is equivalent to shifting each study's estimated HR by 2.31-fold (95% CI, 1.51-2.36). Restricting studies to include only older patients did not modify the results.
Limitations: Limited number of studies and evidence on the absence of publication bias.
Conclusions: Our findings suggest that dialysis initiation considerably reduces mortality among adults with advanced CKD. Future bias-adjusted meta-analyses need to assess outcomes beyond mortality.
Keywords: Dialysis; conservative management; mortality; survival; treatment effects; unmeasured confounding.
© 2020 The Authors.
Figures
References
-
- Centers for Disease Control and Prevention Chronic kidney disease in the United States, 2019. https://www.cdc.gov/kidneydisease/pdf/2019_National-Chronic-Kidney-Disea... Published March 13, 2019. Accessed October 15, 2019.
-
- The Kidney Foundation of Canada Facing the facts: include highlights from the Canadian Organ Replacement Register. https://www.kidney.ca/file/Facing-the-Facts-2018.pdf Published online 2018. Accessed October 14, 2019.
-
- Levey A.S., Coresh J. Chronic kidney disease. Lancet. 2012;379(9811):165–180. - PubMed
-
- Charra B., Calemard E., Ruffet M. Survival as an index of adequacy of dialysis. Kidney Int. 1992;41(5):1286–1291. - PubMed
-
- McIntyre C.W., Rosansky S.J. Starting dialysis is dangerous: how do we balance the risk? Kidney Int. 2012;82(4):382–387. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
