

Melatonin and/or erythropoietin combined with hypothermia in a piglet model of perinatal asphyxia
- PMID: 33604569
- PMCID: PMC7876304
- DOI: 10.1093/braincomms/fcaa211
Melatonin and/or erythropoietin combined with hypothermia in a piglet model of perinatal asphyxia
Abstract
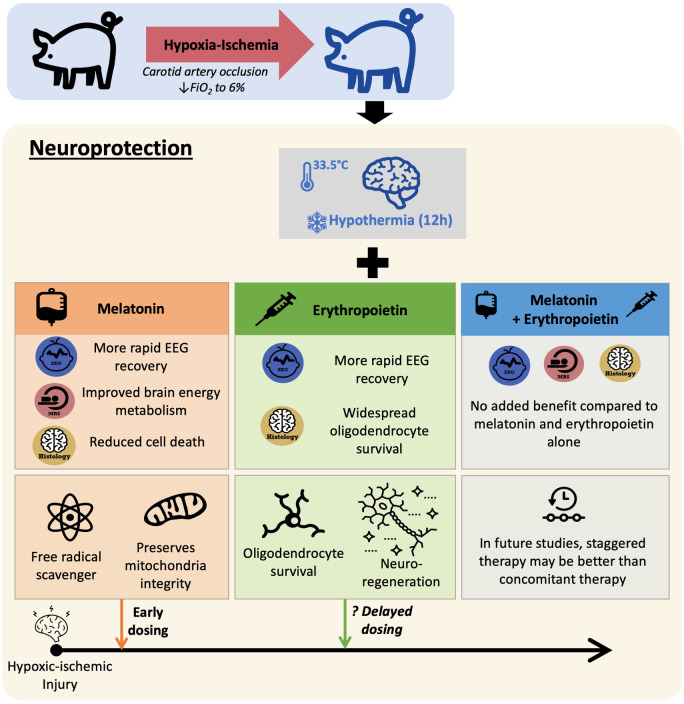
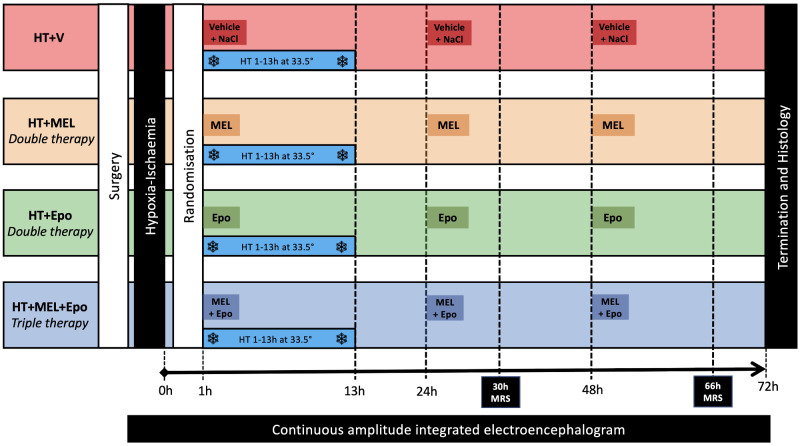
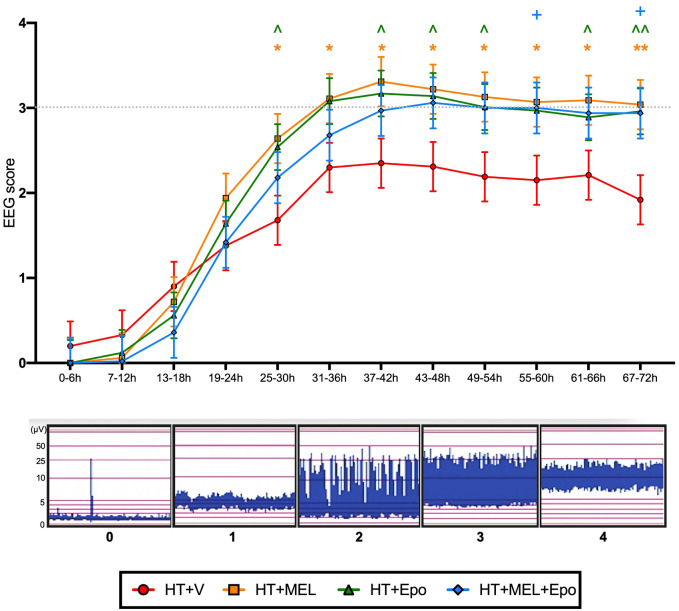
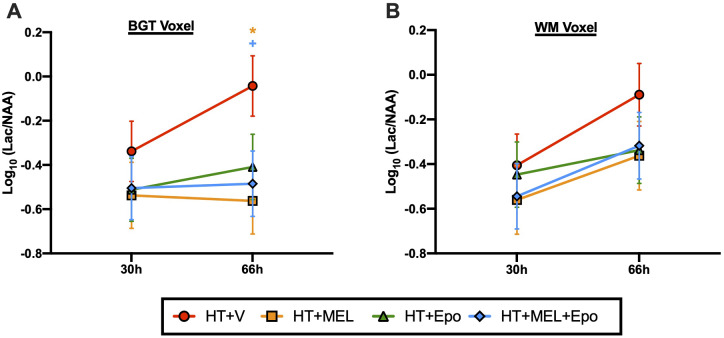
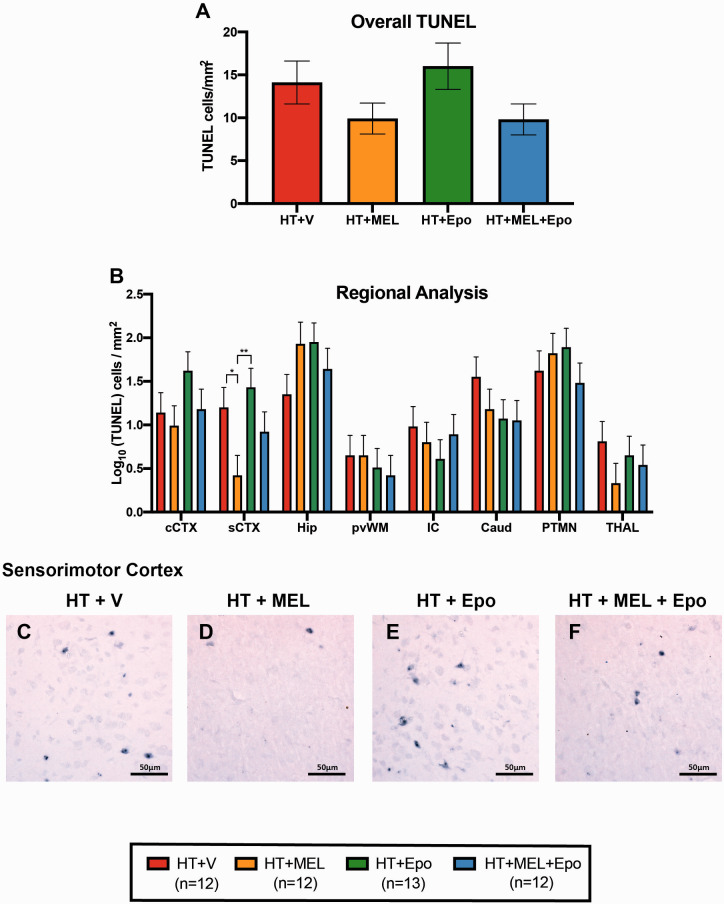
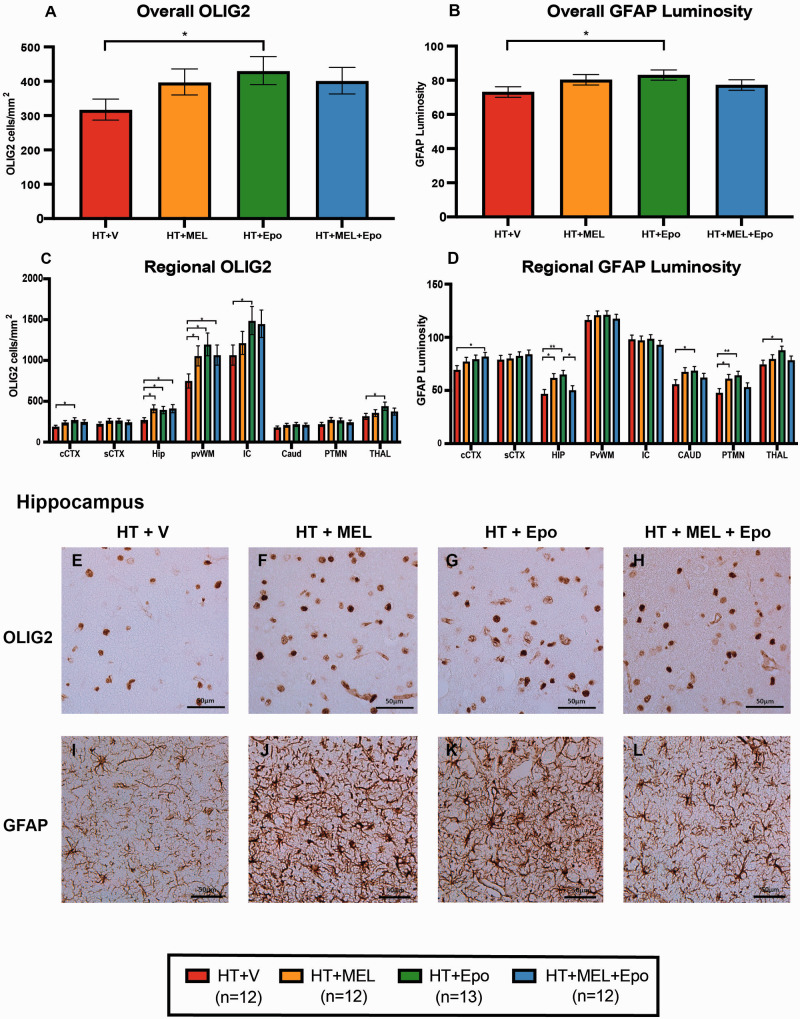
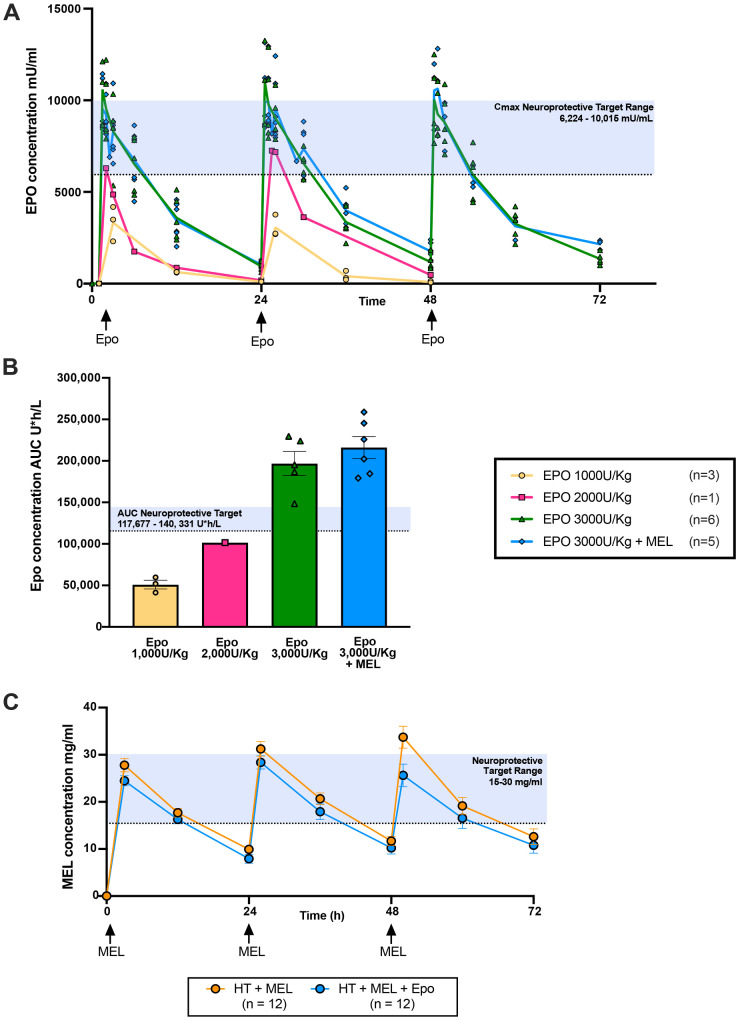
As therapeutic hypothermia is only partially protective for neonatal encephalopathy, safe and effective adjunct therapies are urgently needed. Melatonin and erythropoietin show promise as safe and effective neuroprotective therapies. We hypothesized that melatonin and erythropoietin individually augment 12-h hypothermia (double therapies) and hypothermia + melatonin + erythropoietin (triple therapy) leads to optimal brain protection. Following carotid artery occlusion and hypoxia, 49 male piglets (<48 h old) were randomized to: (i) hypothermia + vehicle (n = 12), (ii) hypothermia + melatonin (20 mg/kg over 2 h) (n = 12), (iii) hypothermia + erythropoietin (3000 U/kg bolus) (n = 13) or (iv) triple therapy (n = 12). Melatonin, erythropoietin or vehicle were given at 1, 24 and 48 h after hypoxia-ischaemia. Hypoxia-ischaemia severity was similar across groups. Therapeutic levels were achieved 3 hours after hypoxia-ischaemia for melatonin (15-30 mg/l) and within 30 min of erythropoietin administration (maximum concentration 10 000 mU/ml). Compared to hypothermia + vehicle, we observed faster amplitude-integrated EEG recovery from 25 to 30 h with hypothermia + melatonin (P = 0.02) and hypothermia + erythropoietin (P = 0.033) and from 55 to 60 h with triple therapy (P = 0.042). Magnetic resonance spectroscopy lactate/N-acetyl aspartate peak ratio was lower at 66 h in hypothermia + melatonin (P = 0.012) and triple therapy (P = 0.032). With hypothermia + melatonin, terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labelled-positive cells were reduced in sensorimotor cortex (P = 0.017) and oligodendrocyte transcription factor 2 labelled-positive counts increased in hippocampus (P = 0.014) and periventricular white matter (P = 0.039). There was no reduction in terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labelled-positive cells with hypothermia + erythropoietin, but increased oligodendrocyte transcription factor 2 labelled-positive cells in 5 of 8 brain regions (P < 0.05). Overall, melatonin and erythropoietin were safe and effective adjunct therapies to hypothermia. Hypothermia + melatonin double therapy led to faster amplitude-integrated EEG recovery, amelioration of lactate/N-acetyl aspartate rise and reduction in terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick-end labelled-positive cells in the sensorimotor cortex. Hypothermia + erythropoietin double therapy was in association with EEG recovery and was most effective in promoting oligodendrocyte survival. Triple therapy provided no added benefit over the double therapies in this 72-h study. Melatonin and erythropoietin influenced cell death and oligodendrocyte survival differently, reflecting distinct neuroprotective mechanisms which may become more visible with longer-term studies. Staggering the administration of therapies with early melatonin and later erythropoietin (after hypothermia) may provide better protection; each therapy has complementary actions which may be time critical during the neurotoxic cascade after hypoxia-ischaemia.
Keywords: erythropoietin; melatonin; neonatal encephalopathy; neuroprotection; therapeutic hypothermia.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Andrabi SA, Sayeed I, Siemen D, Wolf G, Horn TF.. Direct inhibition of the mitochondrial permeability transition pore: a possible mechanism responsible for anti-apoptotic effects of melatonin. FASEB J 2004; 18: 869–71. - PubMed
-
- Azzopardi D, Robertson NJ, Bainbridge A, Cady E, Charles-Edwards G, Deierl A, et al. Moderate hypothermia within 6 h of birth plus inhaled xenon versus moderate hypothermia alone after birth asphyxia (TOBY-Xe): a proof-of-concept, open-label, randomised controlled trial. Lancet Neurol 2016; 15: 145–53. - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials