

Dystonia updates: definition, nomenclature, clinical classification, and etiology
- PMID: 33604773
- PMCID: PMC8099848
- DOI: 10.1007/s00702-021-02314-2
Dystonia updates: definition, nomenclature, clinical classification, and etiology
Abstract
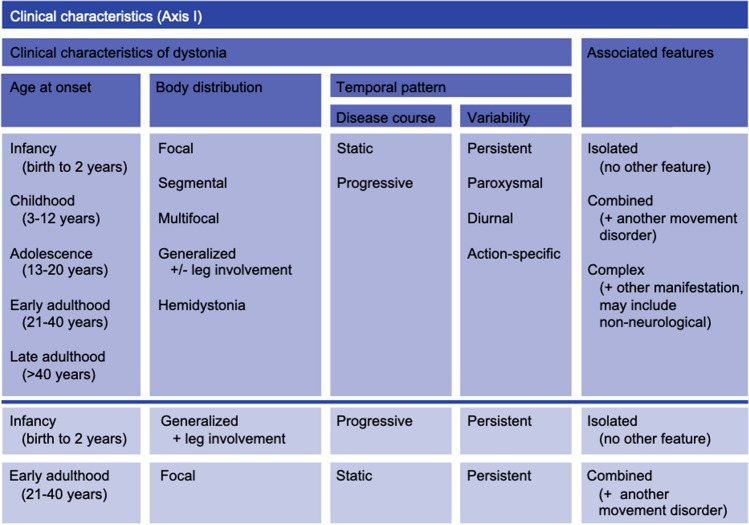
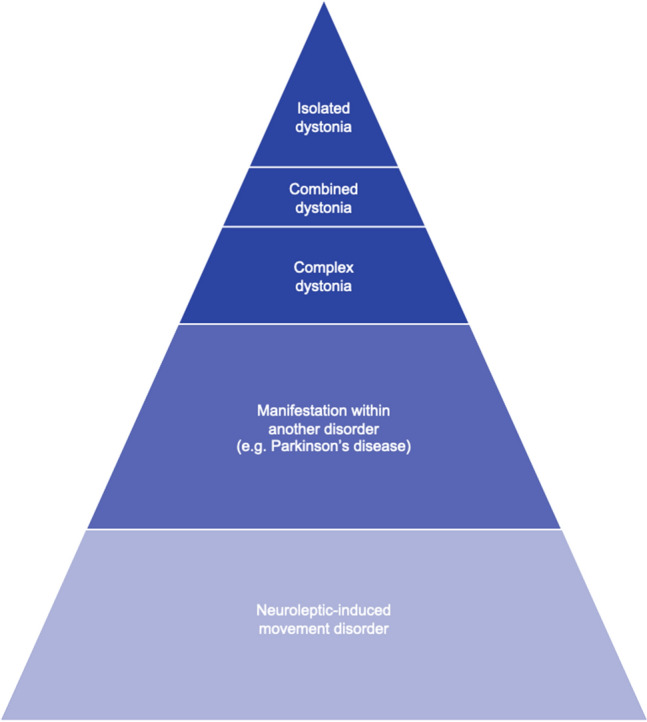
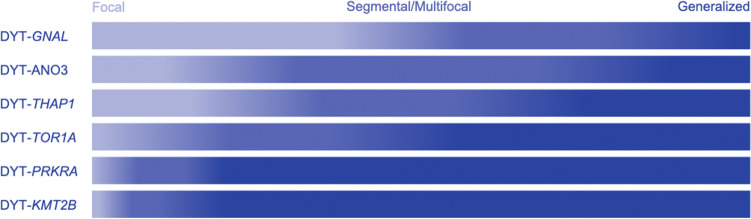
A plethora of heterogeneous movement disorders is grouped under the umbrella term dystonia. The clinical presentation ranges from isolated dystonia to multi-systemic disorders where dystonia is only a co-occurring sign. In the past, definitions, nomenclature, and classifications have been repeatedly refined, adapted, and extended to reflect novel findings and increasing knowledge about the clinical, etiologic, and scientific background of dystonia. Currently, dystonia is suggested to be classified according to two axes. The first axis offers precise categories for the clinical presentation grouped into age at onset, body distribution, temporal pattern and associated features. The second, etiologic, axis discriminates pathological findings, as well as inheritance patterns, mode of acquisition, or unknown causality. Furthermore, the recent recommendations regarding terminology and nomenclature of inherited forms of dystonia and related syndromes are illustrated in this article. Harmonized, specific, and internationally widely used classifications provide the basis for future systematic dystonia research, as well as for more personalized patient counseling and treatment approaches.
Keywords: Clinical classification; Disease etiology; Dystonia; Nomenclature.
Conflict of interest statement
CK serves as a medical advisor to Centogene for genetic testing reports in the fields of movement disorders and dementia, excluding Parkinson’s disease.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
