

Effectiveness, safety and acceptability of no-test medical abortion (termination of pregnancy) provided via telemedicine: a national cohort study
- PMID: 33605016
- PMCID: PMC8360126
- DOI: 10.1111/1471-0528.16668
Effectiveness, safety and acceptability of no-test medical abortion (termination of pregnancy) provided via telemedicine: a national cohort study
Abstract
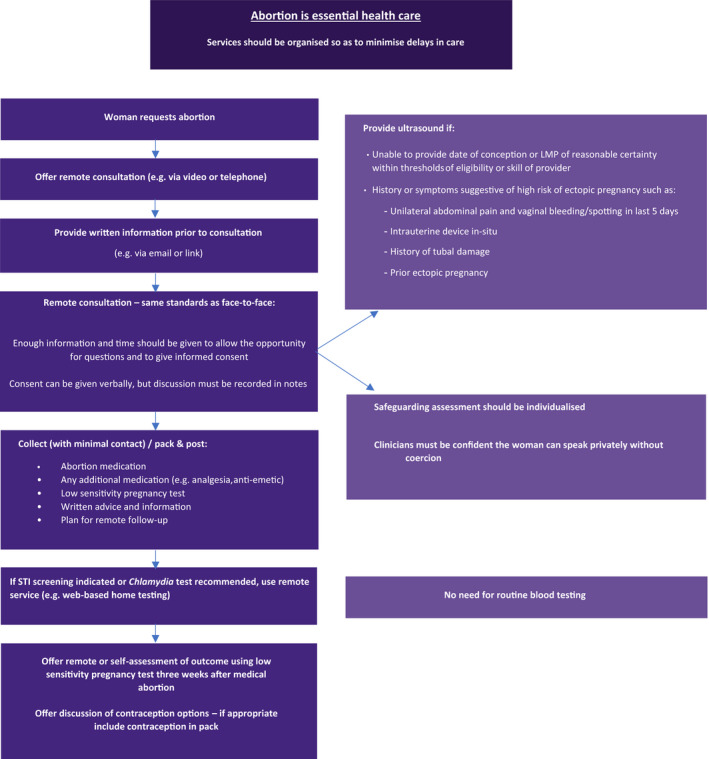
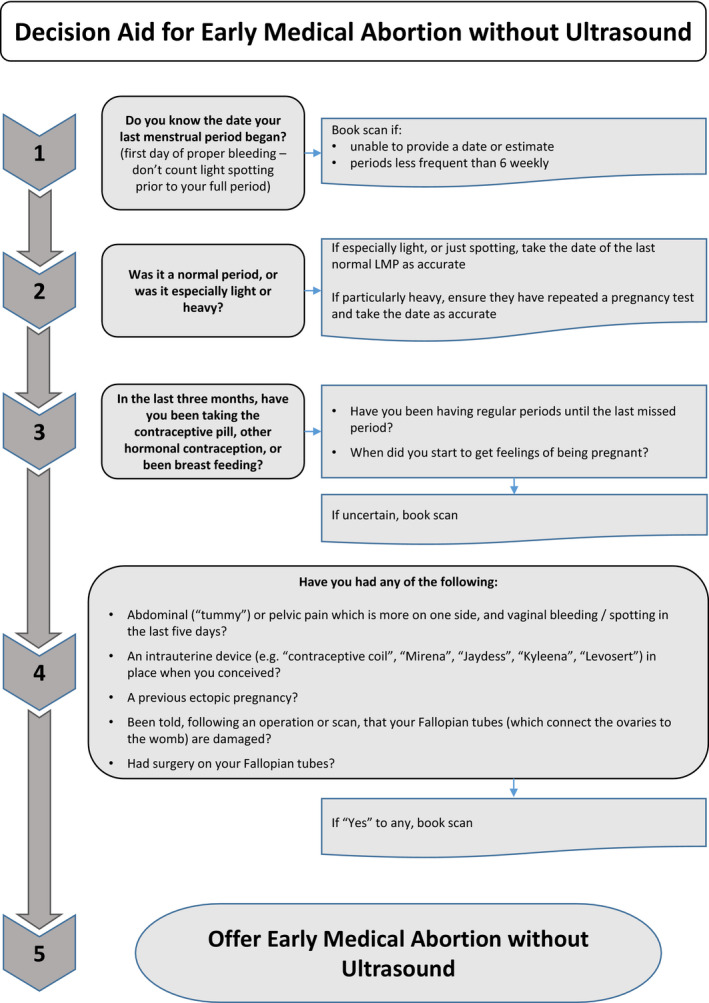
Objective: To compare outcomes before and after implementation of medical abortion (termination of pregnancy) without ultrasound via telemedicine.
Design: Cohort analysis.
Setting: The three main abortion providers.
Population or sample: Medical abortions at home at ≤69 days' gestation in two cohorts: traditional model (in-person with ultrasound, n = 22 158) from January to March 2020 versus telemedicine-hybrid model (either in person or via telemedicine without ultrasound, n = 29 984, of whom 18 435 had no-test telemedicine) between April and June 2020. Sample (n = 52 142) comprises 85% of all medical abortions provided nationally.
Methods: Data from electronic records and incident databases were used to compare outcomes between cohorts, adjusted for baseline differences.
Main outcome measures: Treatment success, serious adverse events, waiting times, gestation at treatment, acceptability.
Results: Mean waiting time from referral to treatment was 4.2 days shorter in the telemedicine-hybrid model and more abortions were provided at ≤6 weeks' gestation (40% versus 25%, P < 0.001). Treatment success (98.8% versus 98.2%, P > 0.999), serious adverse events (0.02% versus 0.04%, P = 0.557) and incidence of ectopic pregnancy (0.2% versus 0.2%, P = 0.796) were not different between models. In the telemedicine-hybrid model, 0.04% were estimated to be over 10 weeks' gestation at the time of the abortion; all were completed safely at home. Within the telemedicine-hybrid model, effectiveness was higher with telemedicine than in-person care (99.2% versus 98.1%, P < 0.001). Acceptability of telemedicine was high (96% satisfied) and 80% reported a future preference for telemedicine.
Conclusions: A telemedicine-hybrid model for medical abortion that includes no-test telemedicine and treatment without an ultrasound is effective, safe, acceptable and improves access to care.
Tweetable abstract: Compelling evidence from 52 142 women shows no-test telemedicine abortion is safe, effective and improves care.
Keywords: Abortion; ambulatory care facilities [N02.278.035]; health planning [N03.349]; induced [E04.520.050]; mifepristone [D04.210.500.365.415.580]; misoprostol [D23.469.700.660.500]; pregnancy complications [C13.703]; telemedicine [N04.590.374.800]; termination of pregnancy.
© 2021 The Authors. BJOG: An International Journal of Obstetrics and Gynaecology published by John Wiley & Sons Ltd.
Figures
Comment in
-
Induced abortion via telemedicine should become the norm: a commentary.BJOG. 2021 Aug;128(9):1475-1476. doi: 10.1111/1471-0528.16740. Epub 2021 Jun 7. BJOG. 2021. PMID: 33982401 No abstract available.
References
-
- Bearak J, Popinchalk A, Ganatra B, Moller A‐B, Tunçalp Ö, Beavin C, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Global Health 2020;8:e1152–61. - PubMed
-
- Regan L, Glasier A. The British 1967 Abortion Act – still fit for purpose? Lancet 2017;390:1936–7. - PubMed
-
- National Institute for Health and Care Excellence (NICE) . Abortion Care. Evidence Review A – Accessibility and Sustainability of Abortion Services. London: National Institute for Health and Care Excellence (NICE); 2019. [www.nice.org.uk/guidance/ng140/documents/evidence‐review]. - PubMed
-
- O’Shea LE, Hawkins JE, Lord J, Schmidt‐Hansen M, Hasler E, Cameron S, et al. Access to and sustainability of abortion services: a systematic review and meta‐analysis for the National Institute of Health and Care Excellence – new clinical guidelines for England. Hum Reprod Update 2020;26:886–903. - PubMed
-
- WHO Global Observatory for eHealth . Telemedicine: Opportunities and Developments in Member States: Report on the Second Global Survey on eHealth. Geneva: World Health Organization; 2010.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
