

Validation of the "Six-and-Twelve" Prognostic Score in Transarterial Chemoembolization-Treated Hepatocellular Carcinoma Patients
- PMID: 33605612
- PMCID: PMC7899857
- DOI: 10.14309/ctg.0000000000000310
Validation of the "Six-and-Twelve" Prognostic Score in Transarterial Chemoembolization-Treated Hepatocellular Carcinoma Patients
Abstract
Introduction: The "six-and-twelve" prognostic score was proposed recently to predict survival rate in patients with unresectable hepatocellular carcinoma (HCC) treated with transarterial chemoembolization (TACE). However, it has not been validated externally. We validated this score and previous prognostic scores in Thai HCC patients treated with TACE.
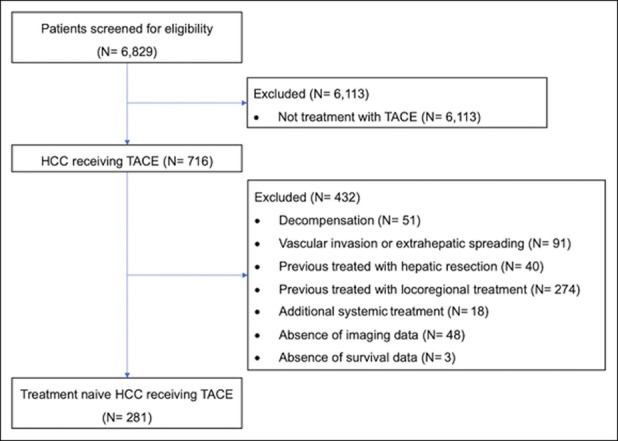
Methods: We identified all HCC patients who underwent TACE between January 2007 and December 2018 at our hospital. The inclusion criteria were treatment-naive, unresectable HCC BCLC-A and BCLC-B; if cirrhosis was present, Child-Pugh score ≤7; and baseline performance status 0-1.
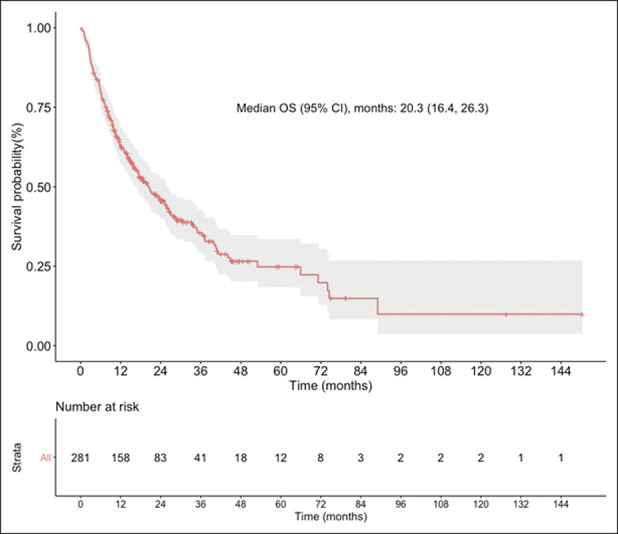
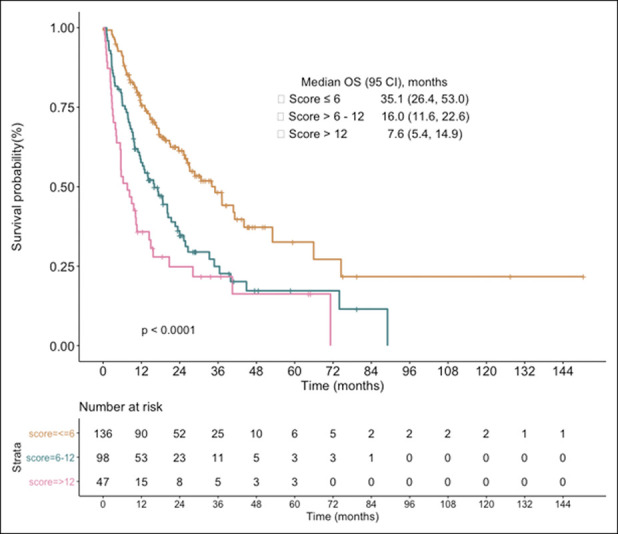
Results: Of 716 HCC patients undergoing TACE, 281 (mean age, 61.1 years; 73.0% men, 92.2% with cirrhosis) were eligible. Approximately half of the patients had hepatitis B virus. Median overall survival was 20.3 (95% confidence interval, 16.4-26.3) months. By stratifying with the "six-and-twelve" score (≤6, >6-12, >12), median (95% confidence interval) overall survival was 35.1 (26.4-53.0), 16.0 (11.6-22.6), and 7.6 (5.4-14.9) months, respectively. Area under the receiver operating characteristic curves (AUROCs) predicting death at 1, 2, and 3 years for the "six-and-twelve" score were 0.714, 0.700, and 0.688, respectively. Compared with the other currently available scores, the AUROC predicting death at 1 year for the "six-and-twelve" score was the most predictive and better than other models except the up-to-seven model.
Discussion: Our study confirms the value of the "six-and-twelve" score to predict survival rate of unresectable HCC treated with TACE. However, in our validation cohort, AUROC of the "six-and-twelve" score was slightly lower than that of the original Chinese cohort (0.73).
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The American College of Gastroenterology.
Conflict of interest statement
Figures
Similar articles
-
Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: A multicentre observational study.J Hepatol. 2019 May;70(5):893-903. doi: 10.1016/j.jhep.2019.01.013. Epub 2019 Jan 18. J Hepatol. 2019. PMID: 30660709
-
Validation and evaluation of clinical prediction systems for first and repeated transarterial chemoembolization in unresectable hepatocellular carcinoma: A Chinese multicenter retrospective study.World J Gastroenterol. 2020 Feb 14;26(6):657-669. doi: 10.3748/wjg.v26.i6.657. World J Gastroenterol. 2020. PMID: 32103874 Free PMC article.
-
Validation of the six-and-twelve criteria among patients with hepatocellular carcinoma and performance score 1 receiving transarterial chemoembolization.World J Gastroenterol. 2020 Apr 21;26(15):1805-1819. doi: 10.3748/wjg.v26.i15.1805. World J Gastroenterol. 2020. PMID: 32351295 Free PMC article.
-
Comparison of transarterial chemoembolization with radiofrequency ablation for unresectable Barcelona Clinic Liver Cancer stage 0/A hepatocellular carcinoma: a propensity score matching.J Gastroenterol Hepatol. 2016 Feb;31(2):442-9. doi: 10.1111/jgh.13077. J Gastroenterol Hepatol. 2016. PMID: 26259976
-
Transarterial chemoembolization in hepatocellular carcinoma treatment: Barcelona clinic liver cancer staging system.World J Gastroenterol. 2015 Sep 28;21(36):10327-35. doi: 10.3748/wjg.v21.i36.10327. World J Gastroenterol. 2015. PMID: 26420959 Free PMC article. Review.
Cited by
-
Decision-Making Scoring System for the Repetition of Conventional Transarterial Chemoembolization in Patients With Inoperable Hepatocellular Carcinoma.Clin Transl Gastroenterol. 2022 Jul 1;13(7):e00506. doi: 10.14309/ctg.0000000000000506. Epub 2022 Jun 1. Clin Transl Gastroenterol. 2022. PMID: 35905418 Free PMC article. Clinical Trial.
-
Enhancing ultrasonographic detection of hepatocellular carcinoma with artificial intelligence: current applications, challenges and future directions.BMJ Open Gastroenterol. 2025 Jul 1;12(1):e001832. doi: 10.1136/bmjgast-2025-001832. BMJ Open Gastroenterol. 2025. PMID: 40592728 Free PMC article. Review.
-
Health-related quality of life in Thai patients with chronic hepatitis B.Gastroenterol Rep (Oxf). 2024 Apr 5;12:goae015. doi: 10.1093/gastro/goae015. eCollection 2024. Gastroenterol Rep (Oxf). 2024. PMID: 38586539 Free PMC article.
-
Comparative performance of the GAAD and ASAP scores in predicting early-stage hepatocellular carcinoma.Gastroenterol Rep (Oxf). 2025 Jul 30;13:goaf074. doi: 10.1093/gastro/goaf074. eCollection 2025. Gastroenterol Rep (Oxf). 2025. PMID: 40746370 Free PMC article.
-
"Six-and-Twelve" Prognostic Score in Transarterial Chemoembolization-Treated Hepatocellular Carcinoma Patients.Cureus. 2023 Nov 28;15(11):e49575. doi: 10.7759/cureus.49575. eCollection 2023 Nov. Cureus. 2023. PMID: 38156124 Free PMC article.
References
-
- Chonprasertsuk S, Vilaichone R. Epidemiology and treatment of hepatocellular carcinoma in Thailand. Jpn J Clin Oncol 2017;47(4):294–7. - PubMed
-
- Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatol Baltim Md 2018;67(1):358–80. - PubMed
-
- Galle PR, Forner A, Llovet JM, et al. EASL clinical practice guidelines: Management of hepatocellular carcinoma. J Hepatol 2018;69(1):182–236. - PubMed
-
- Wang Q, Xia D, Bai W, et al. Development of a prognostic score for recommended TACE candidates with hepatocellular carcinoma: A multicentre observational study. J Hepatol 2019;70(5):893–903. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
