

Comparative Access to and Use of Digital Breast Tomosynthesis Screening by Women's Race/Ethnicity and Socioeconomic Status
- PMID: 33606032
- PMCID: PMC7896194
- DOI: 10.1001/jamanetworkopen.2020.37546
Comparative Access to and Use of Digital Breast Tomosynthesis Screening by Women's Race/Ethnicity and Socioeconomic Status
Abstract
Importance: Digital breast tomosynthesis (DBT) has reduced recall and increased cancer detection compared with digital mammography (DM), depending on women's age and breast density. Whether DBT screening access and use are equitable across groups of women based on race/ethnicity and socioeconomic characteristics is uncertain.
Objective: To determine women's access to and use of DBT screening based on race/ethnicity, educational attainment, and income.
Design, setting, and participants: This cross-sectional study included 92 geographically diverse imaging facilities across 5 US states, at which a total of 2 313 118 screening examinations were performed among women aged 40 to 89 years from January 1, 2011, to December 31, 2017. Data were analyzed from June 13, 2019, to August 18, 2020.
Exposures: Women's race/ethnicity, educational level, and community-level household income.
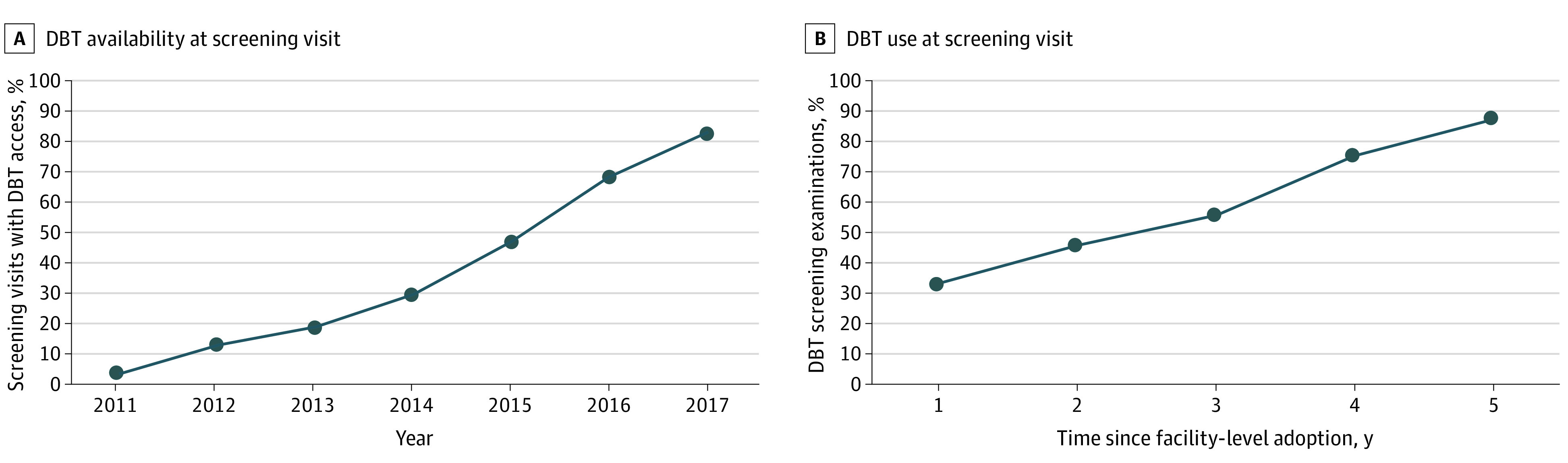
Main outcomes and measures: Access to DBT (on-site access) at time of screening by examination year and actual use of DBT vs DM screening by years since facility-level DBT adoption (≤5 years).
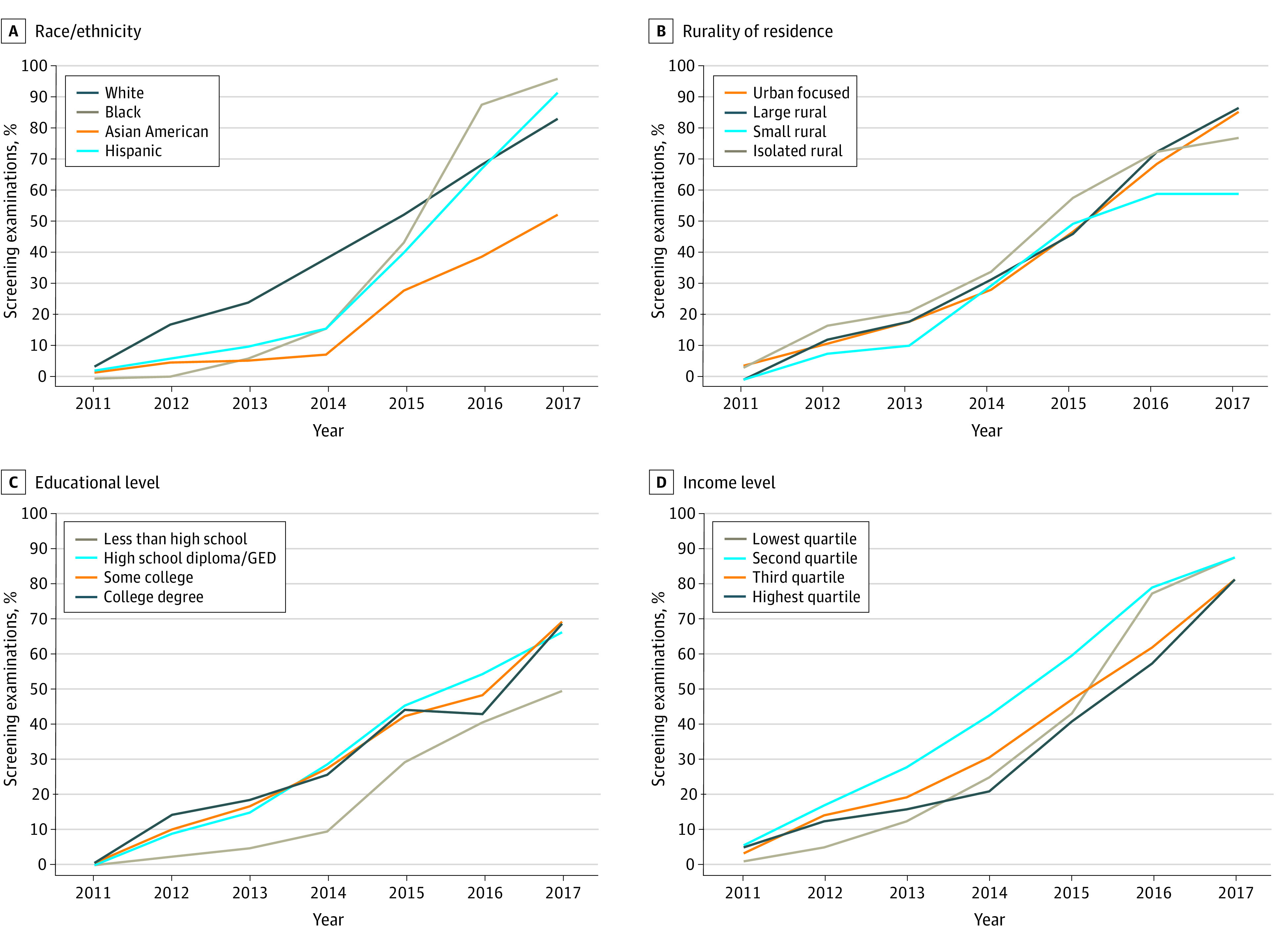
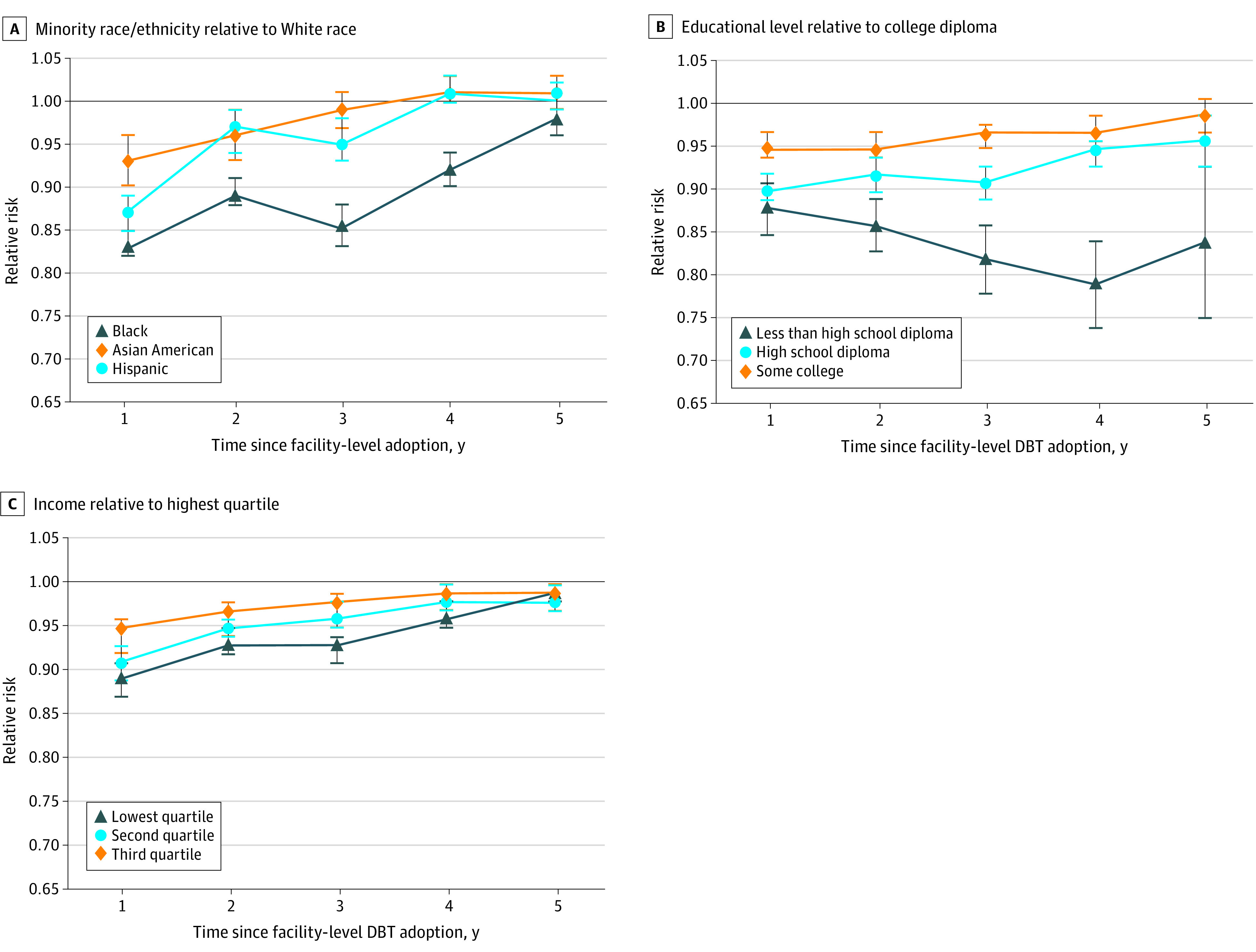
Results: Among the 2 313 118 screening examinations included in the analysis, the proportion of women who had DBT access at the time of their screening appointment increased from 11 558 of 354 107 (3.3%) in 2011 to 194 842 of 235 972 (82.6%) in 2017. In 2012, compared with White women, Black (relative risk [RR], 0.05; 95% CI, 0.03-0.11), Asian American (RR, 0.28; 95% CI, 0.11-0.75), and Hispanic (RR, 0.38; 95% CI, 0.18-0.80) women had significantly less DBT access, and women with less than a high school education had lower DBT access compared with college graduates (RR, 0.18; 95% CI, 0.10-0.32). Among women attending facilities with both DM and DBT available at the time of screening, Black women experienced lower DBT use compared with White women attending the same facility (RRs, 0.83 [95% CI, 0.82-0.85] to 0.98 [95% CI, 0.97-0.99]); women with lower educational level experienced lower DBT use (RRs, 0.79 [95% CI, 0.74-0.84] to 0.88 [95% CI, 0.85-0.91] for non-high school graduates and 0.90 [95% CI, 0.89-0.92] to 0.96 [95% CI, 0.93-0.99] for high school graduates vs college graduates); and women within the lowest income quartile experienced lower DBT use vs women in the highest income quartile (RRs, 0.89 [95% CI, 0.87-0.91] to 0.99 [95% CI, 0.98-1.00]) regardless of the number of years after facility-level DBT adoption.
Conclusions and relevance: In this cross-sectional study, women of minority race/ethnicity and lower socioeconomic status experienced lower DBT access during the early adoption period and persistently lower DBT use when available over time. Future efforts should address racial/ethnic, educational, and financial barriers to DBT screening.
Conflict of interest statement
Figures
Comment in
-
Impact of Race, Ethnicity, and Socioeconomic Status on Digital Breast Tomosynthesis Access and Use.Radiol Imaging Cancer. 2021 Jul;3(4):e219013. doi: 10.1148/rycan.2021219013. Radiol Imaging Cancer. 2021. PMID: 34328351 Free PMC article. No abstract available.
References
-
- Conant EF, Barlow WE, Herschorn SD, et al. ; Population-based Research Optimizing Screening Through Personalized Regimen (PROSPR) Consortium . Association of digital breast tomosynthesis vs digital mammography with cancer detection and recall rates by age and breast density. JAMA Oncol. 2019;5(5):635-642. doi:10.1001/jamaoncol.2018.7078 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
