

Systematic screening for COVID-19 associated invasive aspergillosis in ICU patients by culture and PCR on tracheal aspirate
- PMID: 33606324
- PMCID: PMC8014245
- DOI: 10.1111/myc.13259
Systematic screening for COVID-19 associated invasive aspergillosis in ICU patients by culture and PCR on tracheal aspirate
Abstract
Background: A high prevalence of COVID-19 associated pulmonary aspergillosis (CAPA) has been reported, though histopathological evidence is frequently lacking. To assess the clinical significance of Aspergillus species in respiratory samples of mechanically ventilated COVID-19 patients, we implemented routine screening for Aspergillus in tracheal aspirate (TA).
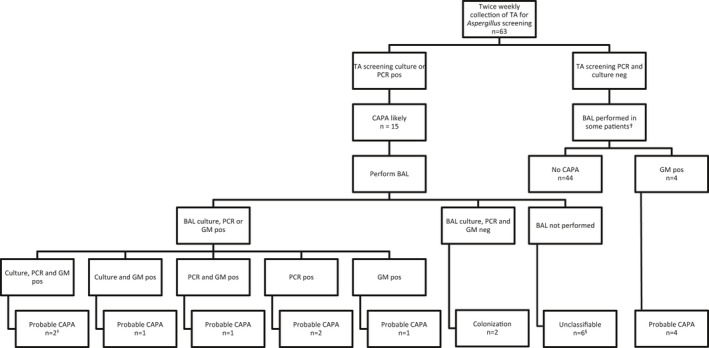
Patients/methods: From all adult COVID-19 patients admitted to the intensive care unit (ICU), TA samples were collected twice a week for Aspergillus screening by PCR and or culture. Bronchoalveolar lavage (BAL) sampling was performed in patients with a positive screening result if possible. Clinical information was obtained from the electronic patient record and patients were categorised according to the recently published consensus case definition for CAPA.
Results: Our study population consisted of 63 predominantly (73%) male patients, with a median age of 62 years and total median ICU stay of 18 days. Aspergillus species were present in TA screening samples from 15 patients (24%), and probable CAPA was diagnosed in 11 (17%) patients. Triazole resistance was detected in one patient (14%). Concordance between TA and BAL was 86%, and all TA culture positives were confirmed in BAL. We were able to withhold treatment in three of fifteen patients with positive screening (20%) but negative BAL results.
Conclusions: Positive culture, molecular detection and or antigen detection of Aspergillus species do not equal infection. Until we understand the clinical relevance of Aspergillus species detected in respiratory samples of COVID-19 patients, minimal-invasive screening by TA is a feasible method to monitor patients. Positive screening results should be an indication to perform a BAL to rule out upper airway colonisation.
Keywords: Aspergillus; COVID-19; COVID-19 associated pulmonary aspergillosis; intensive care unit; invasive fungal infections; invasive pulmonary aspergillosis; screening.
© 2021 The Authors. Mycoses published by Wiley-VCH GmbH.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
