

Fetal, neonatal, and infant outcomes associated with maternal Zika virus infection during pregnancy: A systematic review and meta-analysis
- PMID: 33606729
- PMCID: PMC7894820
- DOI: 10.1371/journal.pone.0246643
Fetal, neonatal, and infant outcomes associated with maternal Zika virus infection during pregnancy: A systematic review and meta-analysis
Abstract
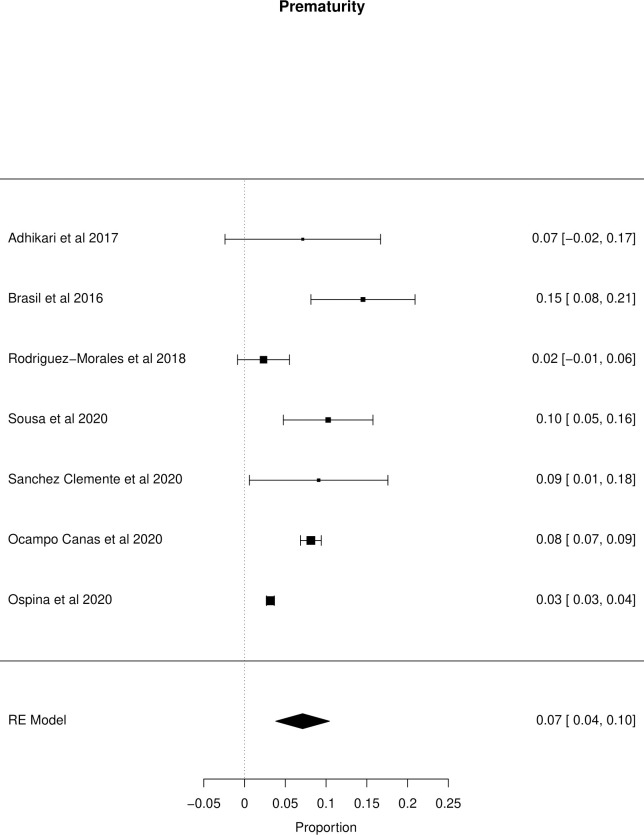
The occurrence of fetal and neonatal disorders in pregnant women with Zika virus infection in the literature is not consistent. This study aims to estimate the prevalence rate of these disorders in fetuses/neonates of pregnant women with confirmed or probable infection by Zika virus. A systematic review with meta-analysis was conducted in November 2020. Cohort studies that contained primary data on the prevalence of unfavorable outcomes in fetuses or neonates of women with confirmed or probable Zika virus infection during pregnancy were included. A total of 21 cohort studies were included, with a total of 35,568 pregnant women. The meta-analysis showed that central nervous system abnormalities had the highest prevalence ratio of 0.06 (95% CI 0.03-0.09). Intracranial calcifications had a prevalence ratio of 0.01 (95% CI 0.01-0.02), and ventriculomegaly 0.01 (95% CI 0.01-0.02). The prevalence ratio of microcephaly was 0.03 (95% CI 0.02-0.05), fetal loss (miscarriage and stillbirth) was 0.04 (95% CI 0.02-0.06), Small for Gestational Age was 0.04 (95% CI 0.00-0,09), Low Birth Weight was 0.05 (95% CI 0.03-0.08) and Prematurity was 0.07 (95% CI 0.04-0.10). The positivity in RT-PCR for ZIKV performed in neonates born to infected mothers during pregnancy was 0.25 (95% CI 0.06-0.44). We also performed the meta-analysis of meta-analysis for microcephaly with the prevalence ratios from other two previously systematic reviews: 0.03 (95% CI 0.00-0.25). Our results contribute to measuring the impact of Zika virus infection during pregnancy on children's health. The continuous knowledge of this magnitude is essential for the implementation development of health initiatives and programs, in addition to promoting disease prevention, especially in the development of a vaccine for Zika virus. PROSPERO protocol registration: http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42019125543.
Conflict of interest statement
NO authors have competing interests.
Figures










References
-
- Ministério da Saúde. Portaria Número 1.813, de 11 de novembro de 2015. [Internet]. 2015 [cited 2020 Feb 5]. Available from: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2015/prt1813_11_11_2015.html.
-
- Kleber de Oliveira W, Cortez-Escalante J, De Oliveira WTGH, do Carmo GMI, Henriques CMP, Coelho GE, et al. Increase in Reported Prevalence of Microcephaly in Infants Born to Women Living in Areas with Confirmed Zika Virus Transmission During the First Trimester of Pregnancy—Brazil, 2015. MMWR Morb Mortal Wkly Rep [Internet]. 2016;65(9):242–7. Available from: http://www.cdc.gov/mmwr/volumes/65/wr/mm6509e2.htm. 10.15585/mmwr.mm6509e2 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
