

Higher severe acute respiratory syndrome coronavirus 2 infection rate in pregnant patients
- PMID: 33607103
- PMCID: PMC7884918
- DOI: 10.1016/j.ajog.2021.02.011
Higher severe acute respiratory syndrome coronavirus 2 infection rate in pregnant patients
Abstract
Background: During the early months of the coronavirus disease 2019 pandemic, risks associated with severe acute respiratory syndrome coronavirus 2 in pregnancy were uncertain. Pregnant patients can serve as a model for the success of clinical and public health responses during public health emergencies as they are typically in frequent contact with the medical system. Population-based estimates of severe acute respiratory syndrome coronavirus 2 infections in pregnancy are unknown because of incomplete ascertainment of pregnancy status or inclusion of only single centers or hospitalized cases. Whether pregnant women were protected by the public health response or through their interactions with obstetrical providers in the early months of pandemic is not clearly understood.
Objective: This study aimed to estimate the severe acute respiratory syndrome coronavirus 2 infection rate in pregnancy and to examine the disparities by race and ethnicity and English language proficiency in Washington State.
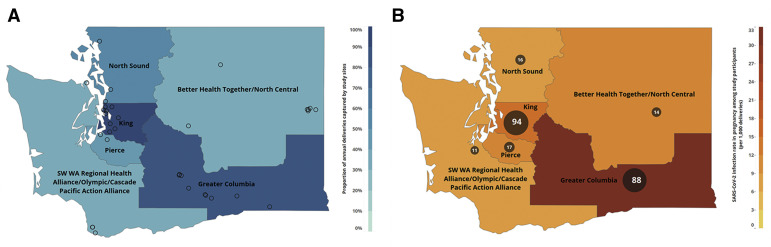
Study design: Pregnant patients with a polymerase chain reaction-confirmed severe acute respiratory syndrome coronavirus 2 infection diagnosed between March 1, 2020, and June 30, 2020 were identified within 35 hospitals and clinics, capturing 61% of annual deliveries in Washington State. Infection rates in pregnancy were estimated overall and by Washington State Accountable Community of Health region and cross-sectionally compared with severe acute respiratory syndrome coronavirus 2 infection rates in similarly aged adults in Washington State. Race and ethnicity and language used for medical care of pregnant patients were compared with recent data from Washington State.
Results: A total of 240 pregnant patients with severe acute respiratory syndrome coronavirus 2 infections were identified during the study period with 70.7% from minority racial and ethnic groups. The principal findings in our study were as follows: (1) the severe acute respiratory syndrome coronavirus 2 infection rate was 13.9 per 1000 deliveries in pregnant patients (95% confidence interval, 8.3-23.2) compared with 7.3 per 1000 (95% confidence interval, 7.2-7.4) in adults aged 20 to 39 years in Washington State (rate ratio, 1.7; 95% confidence interval, 1.3-2.3); (2) the severe acute respiratory syndrome coronavirus 2 infection rate reduced to 11.3 per 1000 deliveries (95% confidence interval, 6.3-20.3) when excluding 45 cases of severe acute respiratory syndrome coronavirus disease 2 detected through asymptomatic screening (rate ratio, 1.3; 95% confidence interval, 0.96-1.9); (3) the proportion of pregnant patients in non-White racial and ethnic groups with severe acute respiratory syndrome coronavirus disease 2 infection was 2- to 4-fold higher than the race and ethnicity distribution of women in Washington State who delivered live births in 2018; and (4) the proportion of pregnant patients with severe acute respiratory syndrome coronavirus 2 infection receiving medical care in a non-English language was higher than estimates of pregnant patients receiving care with limited English proficiency in Washington State (30.4% vs 7.6%).
Conclusion: The severe acute respiratory syndrome coronavirus 2 infection rate in pregnant people was 70% higher than similarly aged adults in Washington State, which could not be completely explained by universal screening at delivery. Pregnant patients from nearly all racial and ethnic minority groups and patients receiving medical care in a non-English language were overrepresented. Pregnant women were not protected from severe acute respiratory syndrome coronavirus 2 infection in the early months of the pandemic. Moreover, the greatest burden of infections occurred in nearly all racial and ethnic minority groups. These data coupled with a broader recognition that pregnancy is a risk factor for severe illness and maternal mortality strongly suggested that pregnant people should be broadly prioritized for coronavirus disease 2019 vaccine allocation in the United States similar to some states.
Keywords: Alaskan Native; American Indian; Black; Hispanic; Pacific Islander; Washington State; coronavirus; coronavirus disease 2019; ethnic disparity; fetus; infection rate; pregnancy; severe acute respiratory syndrome coronavirus 2.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
References
-
- Wiersinga W.J., Rhodes A., Cheng A.C., Peacock S.J., Prescott H.C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;324:782–793. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
