

Diabetic phenotype and prognosis of patients with heart failure and preserved ejection fraction in a real life cohort
- PMID: 33608002
- PMCID: PMC7893869
- DOI: 10.1186/s12933-021-01242-5
Diabetic phenotype and prognosis of patients with heart failure and preserved ejection fraction in a real life cohort
Abstract
Background: Heart failure with preserved ejection fraction (HFpEF) is a heterogeneous syndrome, with several underlying etiologic and pathophysiologic factors. The presence of diabetes might identify an important phenotype, with implications for therapeutic strategies. While diabetes is associated with worse prognosis in HFpEF, the prognostic impact of glycemic control is yet unknown. Hence, we investigated phenotypic differences between diabetic and non-diabetic HFpEF patients (pts), and the prognostic impact of glycated hemoglobin (HbA1C).
Methods: We prospectively enrolled 183 pts with HFpEF (78 ± 9 years, 38% men), including 70 (38%) diabetics (type 2 diabetes only). They underwent 2D echocardiography (n = 183), cardiac magnetic resonance (CMR) (n = 150), and were followed for a combined outcome of all-cause mortality and first HF hospitalization. The prognostic impact of diabetes and glycemic control were determined with Cox proportional hazard models, and illustrated by adjusted Kaplan Meier curves.
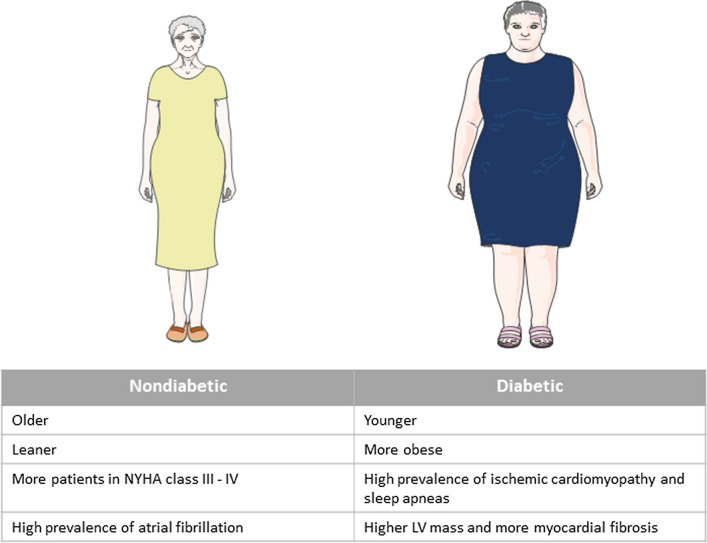
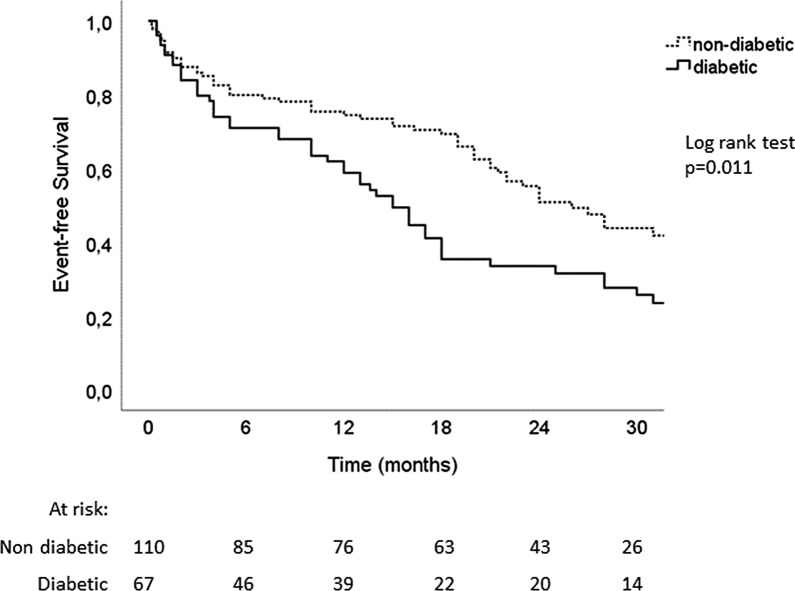
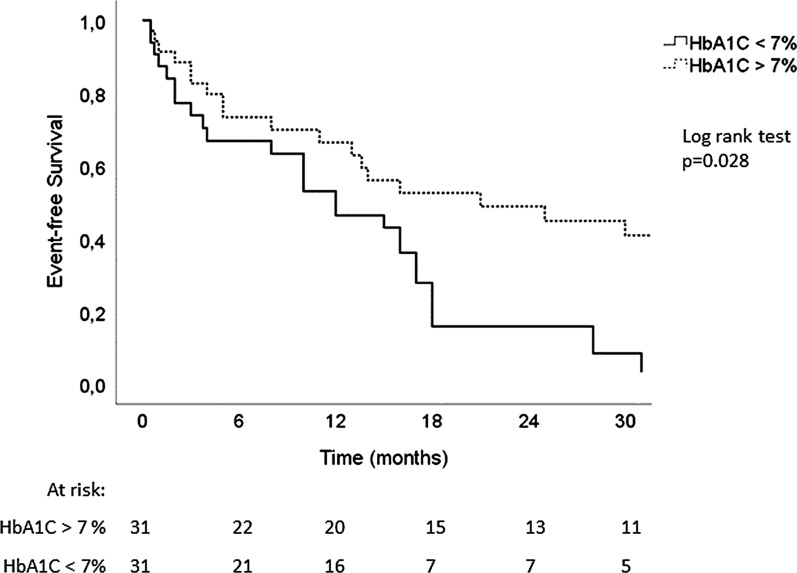
Results: Diabetic HFpEF pts were younger (76 ± 9 vs 80 ± 8 years, p = 0.002), more obese (BMI 31 ± 6 vs 27 ± 6 kg/m2, p = 0.001) and suffered more frequently from sleep apnea (18% vs 7%, p = 0.032). Atrial fibrillation, however, was more frequent in non-diabetic pts (69% vs 53%, p = 0.028). Although no echocardiographic difference could be detected, CMR analysis revealed a trend towards higher LV mass (66 ± 18 vs 71 ± 14 g/m2, p = 0.07) and higher levels of fibrosis (53% vs 36% of patients had ECV by T1 mapping > 33%, p = 0.05) in diabetic patients. Over 25 ± 12 months, 111 HFpEF pts (63%) reached the combined outcome (24 deaths and 87 HF hospitalizations). Diabetes was a significant predictor of mortality and hospitalization for heart failure (HR: 1.72 [1.1-2.6], p = 0.011, adjusted for age, BMI, NYHA class and renal function). In diabetic patients, lower levels of glycated hemoglobin (HbA1C < 7%) were associated with worse prognosis (HR: 2.07 [1.1-4.0], p = 0.028 adjusted for age, BMI, hemoglobin and NT-proBNP levels).
Conclusion: Our study highlights phenotypic features characterizing diabetic patients with HFpEF. Notably, they are younger and more obese than their non-diabetic counterpart, but suffer less from atrial fibrillation. Although diabetes is a predictor of poor outcome in HFpEF, intensive glycemic control (HbA1C < 7%) in diabetic patients is associated with worse prognosis.
Keywords: HbA1C; Heart failure and preserved ejection fraction; Prognosis; Type 2 diabetes.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Anker SD, Butler J, Filippatos GS, Jamal W, Salsali A, Schnee J, et al. Evaluation of the effects of sodium-glucose co-transporter 2 inhibition with empagliflozin on morbidity and mortality in patients with chronic heart failure and a preserved ejection fraction: rationale for and design of the EMPEROR-Preserved Trial. Eur J Heart Fail. 2019;21(10):1279–1287. doi: 10.1002/ejhf.1596. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
