

Asthma-related inflammation promotes lung metastasis of breast cancer cells through CCL11-CCR3 pathway
- PMID: 33608009
- PMCID: PMC7893955
- DOI: 10.1186/s12931-021-01652-9
Asthma-related inflammation promotes lung metastasis of breast cancer cells through CCL11-CCR3 pathway
Abstract
Background: Mechanisms that preclude lung metastasis are still barely understood. The possible consequences of allergic airways inflammation on cancer dissemination were studied in a mouse model of breast cancer.
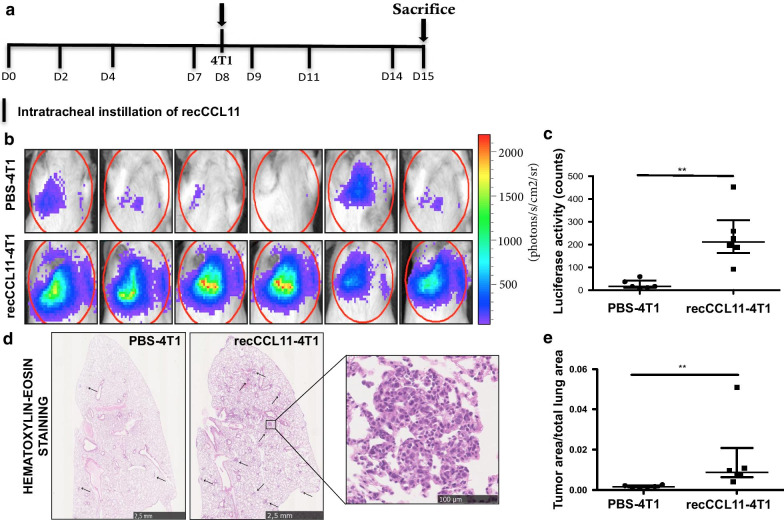
Methods: Balb/c mice were immunized and daily exposed to ovalbumin (OVA) from day 21. They were subcutaneously injected with 4T1 mammary tumor cells on day 45 and sacrificed on day 67. Lung metastases were measured by biophotonic imaging (IVIS® 200 Imaging System) and histological measurement of tumor area (Cytomine software). Effects of CCL11 were assessed in vivo by intratracheal instillations of recCCL11 and in vitro using Boyden chambers. CCR3 expression on cell surface was assessed by flow cytometry.
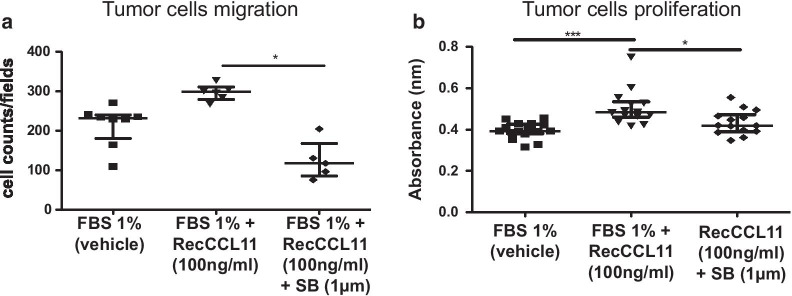
Results: The extent of tumor metastases was significantly higher in lungs of OVA-exposed mice and increased levels of CCL11 expression were measured after OVA exposure. Migration of 4T1 cells and neutrophils was stimulated in vitro and in vivo by recCCL11. 4T1 cells and neutrophils express CCR3 as shown by flow cytometry and a selective CCR3 antagonist (SB-297006) inhibited the induction of 4T1 cells migration and proliferation in response to recCCL11.
Conclusions: Allergic inflammation generated by exposure to allergens triggers the implantation of metastatic cells from primary breast tumor into lung tissues plausibly in a CCL11-CCR3-dependent manner. This indicates that asthma related inflammation in lungs might be a risk factor for lung metastasis in breast cancer patients.
Keywords: Asthma; Breast cancer; CCL11–CCR3; Lung inflammation; Lung metastasis.
Conflict of interest statement
DC is the founder of Aquilon Pharmaceuticals, received speaker fees from AstraZeneca, Boehringer-Ingelheim, Chiesi and GSK and received consultancy fees from AstraZeneca, Boehringer-Ingelheim, Chiesi and Sanofi for the participation to advisory boards. None of these activities have any connection with oncology or development of drugs in the field of oncology.
Figures


Similar articles
-
The airway smooth muscle CCR3/CCL11 axis is inhibited by mast cells.Allergy. 2008 Sep;63(9):1148-55. doi: 10.1111/j.1398-9995.2008.01684.x. Allergy. 2008. PMID: 18699931 Free PMC article.
-
Catalpol alleviates ovalbumin-induced asthma in mice: Reduced eosinophil infiltration in the lung.Int Immunopharmacol. 2017 Feb;43:140-146. doi: 10.1016/j.intimp.2016.12.011. Epub 2016 Dec 16. Int Immunopharmacol. 2017. PMID: 27992791
-
Expression and effects of IL-33 and ST2 in allergic bronchial asthma: IL-33 induces eotaxin production in lung fibroblasts.Int Arch Allergy Immunol. 2011;155 Suppl 1:12-20. doi: 10.1159/000327259. Epub 2011 Jun 1. Int Arch Allergy Immunol. 2011. PMID: 21646790
-
Upregulation of CCR3 by age-related stresses promotes choroidal endothelial cell migration via VEGF-dependent and -independent signaling.Invest Ophthalmol Vis Sci. 2011 Oct 21;52(11):8271-7. doi: 10.1167/iovs.11-8230. Invest Ophthalmol Vis Sci. 2011. PMID: 21917937 Free PMC article.
-
Emerging Roles of C-C Motif Ligand 11 (CCL11) in Cancers and Liver Diseases: Mechanisms and Therapeutic Implications.Int J Mol Sci. 2025 May 13;26(10):4662. doi: 10.3390/ijms26104662. Int J Mol Sci. 2025. PMID: 40429807 Free PMC article. Review.
Cited by
-
The twilight zone: plasticity and mixed ontogeny of neutrophil and eosinophil granulocyte subsets.Semin Immunopathol. 2021 Jun;43(3):337-346. doi: 10.1007/s00281-021-00862-z. Epub 2021 May 19. Semin Immunopathol. 2021. PMID: 34009400 Free PMC article. Review.
-
The elusive Luminal B breast cancer and the mysterious chemokines.J Cancer Res Clin Oncol. 2023 Nov;149(14):12807-12819. doi: 10.1007/s00432-023-05094-2. Epub 2023 Jul 17. J Cancer Res Clin Oncol. 2023. PMID: 37458802 Free PMC article.
-
The Use of Biologics for Targeting GPCRs in Metastatic Cancers.BioTech (Basel). 2025 Jan 30;14(1):7. doi: 10.3390/biotech14010007. BioTech (Basel). 2025. PMID: 39982274 Free PMC article. Review.
-
Role of the "inflammation-immunity-metabolism" network in non-small cell lung cancer: a multi-omics analysis.Discov Oncol. 2025 May 21;16(1):847. doi: 10.1007/s12672-025-02692-z. Discov Oncol. 2025. PMID: 40397292 Free PMC article.
-
The Association of Blood Eosinophils and Neutrophils Expressing Eosinophilic Surface Markers with the Severity and Outcome of COVID-19.Microorganisms. 2024 Dec 4;12(12):2503. doi: 10.3390/microorganisms12122503. Microorganisms. 2024. PMID: 39770705 Free PMC article.
References
-
- Jacobsen EA, Ochkur SI, Doyle AD, LeSuer WE, Li W, Protheroe CA, Colbert D, Zellner KR, Shen HH, Irvin CG, et al. Lung pathologies in a chronic inflammation mouse model are independent of eosinophil degranulation. Am J Respir Crit Care Med. 2017;195:1321–1332. doi: 10.1164/rccm.201606-1129OC. - DOI - PMC - PubMed
-
- Rosenberger A, Bickeboller H, McCormack V, Brenner DR, Duell EJ, Tjonneland A, Friis S, Muscat JE, Yang P, Wichmann HE, et al. Asthma and lung cancer risk: a systematic investigation by the International Lung Cancer Consortium. Carcinogenesis. 2012;33:587–597. doi: 10.1093/carcin/bgr307. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
