

Development of genome-wide polygenic risk scores for lipid traits and clinical applications for dyslipidemia, subclinical atherosclerosis, and diabetes cardiovascular complications among East Asians
- PMID: 33608049
- PMCID: PMC7893928
- DOI: 10.1186/s13073-021-00831-z
Development of genome-wide polygenic risk scores for lipid traits and clinical applications for dyslipidemia, subclinical atherosclerosis, and diabetes cardiovascular complications among East Asians
Abstract
Background: The clinical utility of personal genomic information in identifying individuals at increased risks for dyslipidemia and cardiovascular diseases remains unclear.
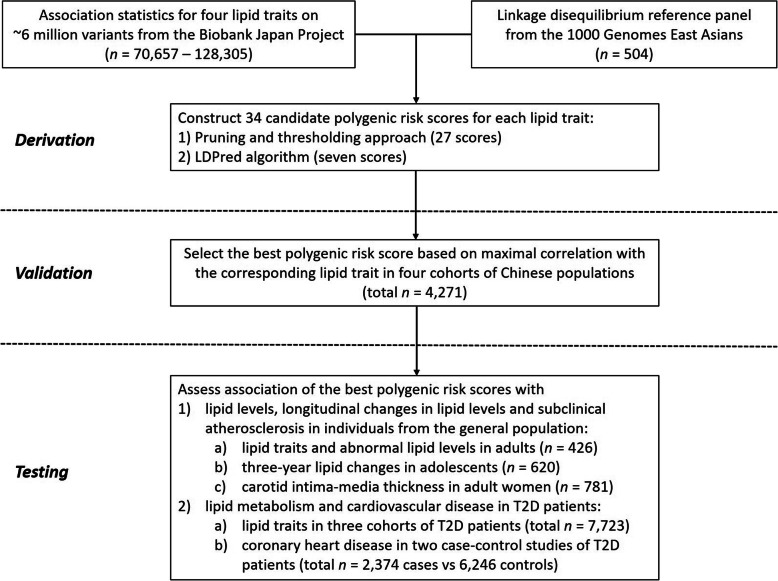
Methods: We used data from Biobank Japan (n = 70,657-128,305) and developed novel East Asian-specific genome-wide polygenic risk scores (PRSs) for four lipid traits. We validated (n = 4271) and subsequently tested associations of these scores with 3-year lipid changes in adolescents (n = 620), carotid intima-media thickness (cIMT) in adult women (n = 781), dyslipidemia (n = 7723), and coronary heart disease (CHD) (n = 2374 cases and 6246 controls) in type 2 diabetes (T2D) patients.
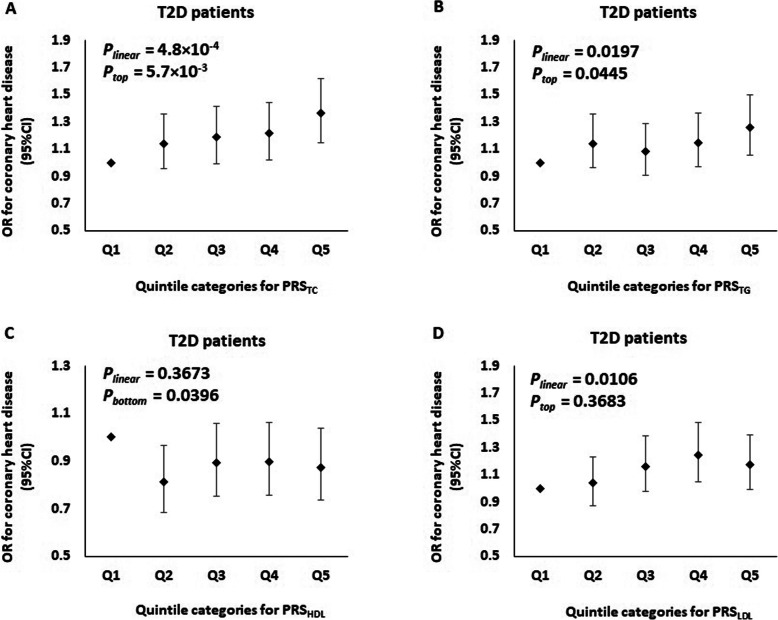
Results: Our PRSs aggregating 84-549 genetic variants (0.251 < correlation coefficients (r) < 0.272) had comparably stronger association with lipid variations than the typical PRSs derived based on the genome-wide significant variants (0.089 < r < 0.240). Our PRSs were robustly associated with their corresponding lipid levels (7.5 × 10- 103 < P < 1.3 × 10- 75) and 3-year lipid changes (1.4 × 10- 6 < P < 0.0130) which started to emerge in childhood and adolescence. With the adjustments for principal components (PCs), sex, age, and body mass index, there was an elevation of 5.3% in TC (β ± SE = 0.052 ± 0.002), 11.7% in TG (β ± SE = 0.111 ± 0.006), 5.8% in HDL-C (β ± SE = 0.057 ± 0.003), and 8.4% in LDL-C (β ± SE = 0.081 ± 0.004) per one standard deviation increase in the corresponding PRS. However, their predictive power was attenuated in T2D patients (0.183 < r < 0.231). When we included each PRS (for TC, TG, and LDL-C) in addition to the clinical factors and PCs, the AUC for dyslipidemia was significantly increased by 0.032-0.057 in the general population (7.5 × 10- 3 < P < 0.0400) and 0.029-0.069 in T2D patients (2.1 × 10- 10 < P < 0.0428). Moreover, the quintile of TC-related PRS was moderately associated with cIMT in adult women (β ± SE = 0.011 ± 0.005, Ptrend = 0.0182). Independent of conventional risk factors, the quintile of PRSs for TC [OR (95% CI) = 1.07 (1.03-1.11)], TG [OR (95% CI) = 1.05 (1.01-1.09)], and LDL-C [OR (95% CI) = 1.05 (1.01-1.09)] were significantly associated with increased risk of CHD in T2D patients (4.8 × 10- 4 < P < 0.0197). Further adjustment for baseline lipid drug use notably attenuated the CHD association.
Conclusions: The PRSs derived and validated here highlight the potential for early genomic screening and personalized risk assessment for cardiovascular disease.
Keywords: Diabetes cardiovascular complications; East Asians; Lipid traits; Polygenic risk scores; Subclinical atherosclerosis.
Conflict of interest statement
J.C.N.C reported receiving grants and/or honoraria for consultancy or giving lectures from AstraZeneca, Bayer, Bristol-Myers Squibb, Boehringer Ingelheim, Daiichi-Sankyo, Eli-Lilly, GlaxoSmithKline, Merck Serono, Merck Sharp & Dohme, Novo Nordisk, Pfizer, and Sanofi. A.P.S.K reported receiving research grants and/or honoraria from Abbott, Astra Zeneca, Eli-Lilly, Merck Serono, Nestle, Novo Nordisk, and Sanofi. R.C.W.M reported having received research grants for clinical trials from AstraZeneca, Bayer, MSD, Novo Nordisk, Sanofi, Tricida Inc. and honoraria for consultancy or lectures from AstraZeneca, and Boehringer Ingelheim. JCNC, WYS, RCWM and CKPL are founding members of GemVCare, a technology start-up initiated with support from the Hong Kong Government Innovation and Technology Commission and its Technology Start-up Support Scheme for Universities (TSSSU). The remaining authors declare that they have no competing interests.
Figures
Similar articles
-
Polygenic risk scores for the prediction of common cancers in East Asians: A population-based prospective cohort study.Elife. 2023 Mar 27;12:e82608. doi: 10.7554/eLife.82608. Elife. 2023. PMID: 36971353 Free PMC article.
-
Predictive Utility of Polygenic Risk Scores for Coronary Heart Disease in Three Major Racial and Ethnic Groups.Am J Hum Genet. 2020 May 7;106(5):707-716. doi: 10.1016/j.ajhg.2020.04.002. Am J Hum Genet. 2020. PMID: 32386537 Free PMC article.
-
Coronary heart disease and ischemic stroke polygenic risk scores and atherosclerotic cardiovascular disease in a diverse, population-based cohort study.PLoS One. 2023 Jun 16;18(6):e0285259. doi: 10.1371/journal.pone.0285259. eCollection 2023. PLoS One. 2023. PMID: 37327218 Free PMC article.
-
Implementing Reporting Standards for Polygenic Risk Scores for Atherosclerotic Cardiovascular Disease.Curr Atheroscler Rep. 2023 Jun;25(6):323-330. doi: 10.1007/s11883-023-01104-3. Epub 2023 May 24. Curr Atheroscler Rep. 2023. PMID: 37223852 Free PMC article. Review.
-
Polygenic risk scores for the diagnosis and management of dyslipidemia.Curr Opin Endocrinol Diabetes Obes. 2022 Apr 1;29(2):95-100. doi: 10.1097/MED.0000000000000708. Curr Opin Endocrinol Diabetes Obes. 2022. PMID: 35034034 Review.
Cited by
-
Racial and ethnic influences on carotid atherosclerosis: Epidemiology and risk factors.SAGE Open Med. 2024 Jun 23;12:20503121241261840. doi: 10.1177/20503121241261840. eCollection 2024. SAGE Open Med. 2024. PMID: 39045542 Free PMC article. Review.
-
DNA methylation markers for kidney function and progression of diabetic kidney disease.Nat Commun. 2023 May 15;14(1):2543. doi: 10.1038/s41467-023-37837-7. Nat Commun. 2023. PMID: 37188670 Free PMC article.
-
Associations between the Genetic Heritability of Dyslipidemia and Dietary Patterns in Korean Adults Based on Sex Differences.Nutrients. 2023 Oct 16;15(20):4385. doi: 10.3390/nu15204385. Nutrients. 2023. PMID: 37892463 Free PMC article.
-
Lipids dysregulation in diseases: core concepts, targets and treatment strategies.Lipids Health Dis. 2025 Feb 21;24(1):61. doi: 10.1186/s12944-024-02425-1. Lipids Health Dis. 2025. PMID: 39984909 Free PMC article. Review.
-
Assessing the safety of lipid-modifying medications among Chinese adolescents: a drug-target Mendelian randomization study.BMC Med. 2023 Oct 31;21(1):410. doi: 10.1186/s12916-023-03115-y. BMC Med. 2023. PMID: 37904165 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
