

Real-life use of talimogene laherparepvec (T-VEC) in melanoma patients in centers in Austria, Switzerland and Germany
- PMID: 33608376
- PMCID: PMC7898852
- DOI: 10.1136/jitc-2020-001701
Real-life use of talimogene laherparepvec (T-VEC) in melanoma patients in centers in Austria, Switzerland and Germany
Erratum in
-
Correction: Real-life use of talimogene laherparepvec (T-VEC) in melanoma patients in centers in Austria, Switzerland and Germany.J Immunother Cancer. 2021 Oct;9(10):e001701corr1. doi: 10.1136/jitc-2020-001701corr1. J Immunother Cancer. 2021. PMID: 34645676 Free PMC article. No abstract available.
Abstract
Background: Talimogene laherparepvec (T-VEC) is a licensed therapy for use in melanoma patients of stage IIIB-IVM1a with injectable, unresectable metastatic lesions in Europe. Approval was based on the Oncovex Pivotal Trial in Melanoma study, which also included patients with distant metastases and demonstrated an overall response rate (ORR) of 40.5% and a complete response (CR) rate of 16.6%.
Objectives: The aim of this study was to assess the outcome of melanoma patients treated with T-VEC in a real-life clinical setting.
Methods: Based on data from 10 melanoma centers in Austria, Switzerland and southern Germany, we conducted a retrospective chart review, which included 88 patients (44 male, 44 female) with a median age of 72 years (range 36-95 years) treated with T-VEC during the period from May 2016 to January 2020.
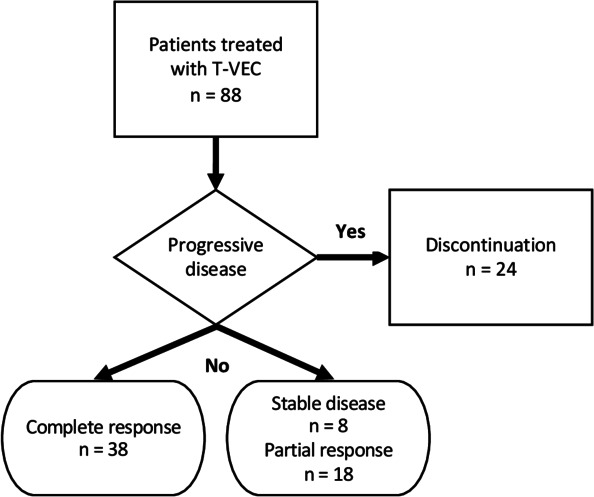
Results: 88 patients fulfilled the inclusion criteria for analysis. The ORR was 63.7%. 38 patients (43.2%) showed a CR, 18 (20.5%) had a partial response, 8 (9.1%) had stable disease and 24 (27.3%) patients had a progressive disease. The median treatment period was 19 weeks (range: 1-65), an average of 11 doses (range: 1-36) were applied. 39 (45.3%) patients developed adverse events, mostly mild, grade I (64.1%).
Conclusion: This real-life cohort treatment with T-VEC showed a high ORR and a large number of durable CRs.
Keywords: immunotherapy; melanoma; oncolytic virotherapy; oncolytic viruses.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: JMR received project funding by Amgen, Speakers bureau of Amgen and Bristol Myers Squibb and travel support from Bristol Myers Squibb, Pierre Fabre outside of the submitted work. JMR has intermittent project focused consultant or advisory relationships with Merck/Pfizer, Merck Sharp & Dohme, Amgen, Novartis, Bristol Myers and Squibb and Pierre Fabre and has received travel support from Ultrasun, L’ oreal, Merck Sharp & Dohme, Bristol Myers and Squibb and Pierre Fabre outside of the submitted work. PK has received honoraria for travel/congress support and consulting/advisory roles for Roche, Bristol Myers Squibb (BMS), Merck Sharp and Dome (MSD), Novartis, Amgen, Pierre Fabre and Sanofi Aventis unrelated to the submitted work. ER Honoraria, consulting or advisory role: Amgen, Bayer, Bristol Myers Squibb, MSD, Merck, Novartis, Pierre Fabre, Roche, SanofiSpeakers'bureau: Amgen, Bristol Myers Squibb, MSD, Merck, Novartis, Pierre Fabre, SanofiResearch funding site PI: Amgen, Bristol Myers Squibb, MSD, Novartis, Pierre Fabre, Roche Research funding steering committee: Novartistravel, accommodations, expenses: Amgen, Bristol Myers Squibb, MSD, Merck, Novartis, Pierre Fabre, Roche, Sanofi. CH is associated with consulting or advisory role for Bristol-Myers Squibb, Amgen, Merck Sharp and Dohme, Novartis, Pierre Fabre and Speaker’s bureau of Bristol-Myers Squibb, Amgen, Merck Sharp & Dohme, Pierre Fabre and received travel/accommodations/expenses from Amgen, Bristol-Myers Squibb, Merck Sharp and Dohme, Pierre Fabre.C.HO. is associated with advisory role for Advisory Boards: Amgen, Astra Zeneca, BMS, Inzyte, MSD, Novartis, Pierre Fabre, Roche and Speakers bureau of Amgen, BMS, MSD, Novartis, Roche.
Figures





References
-
- Andtbacka RHI, Agarwala SS, Ollila DW, et al. . Cutaneous head and neck melanoma in OPTiM, a randomized phase 3 trial of talimogene laherparepvec versus granulocyte-macrophage colony-stimulating factor for the treatment of unresected stage IIIB/IIIC/IV melanoma. Head Neck 2016;38:1752–8. 10.1002/hed.24522 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical