

Use of pembrolizumab with or without pomalidomide in HIV-associated non-Hodgkin's lymphoma
- PMID: 33608378
- PMCID: PMC7898875
- DOI: 10.1136/jitc-2020-002097
Use of pembrolizumab with or without pomalidomide in HIV-associated non-Hodgkin's lymphoma
Abstract
Background: Non-Hodgkin's lymphoma (NHL) is currently the most common malignancy among people living with HIV (PLWH) in the USA. NHL in PLWH is more frequently associated with oncogenic viruses than NHL in immunocompetent individuals and is generally associated with increased PD-1 expression and T cell exhaustion. An effective immune-based second-line approach that is less immunosuppressive than chemotherapy may decrease infection risk, improve immune control of oncogenic viruses, and ultimately allow for better lymphoma control.
Methods: We conducted a retrospective study of patients with HIV-associated lymphomas treated with pembrolizumab±pomalidomide in the HIV and AIDS Malignancy Branch, Center for Cancer Research, National Cancer Institute.
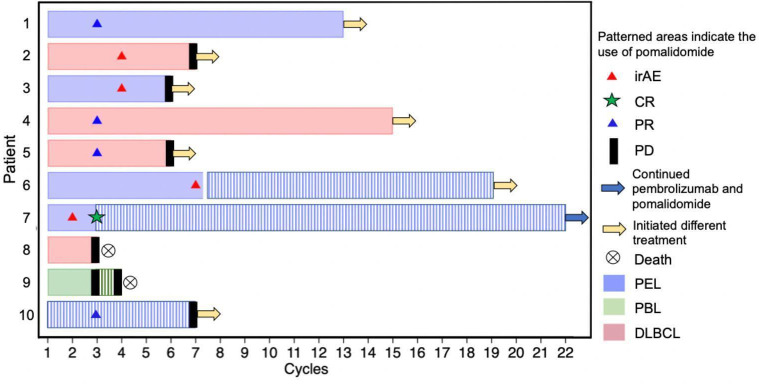
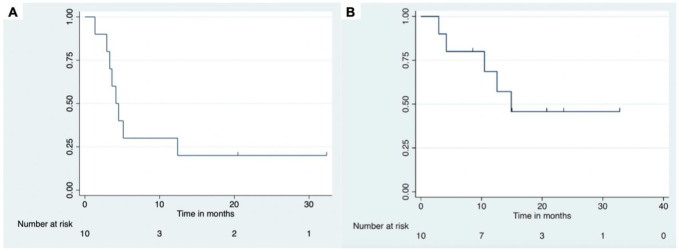
Results: We identified 10 patients with stage IV relapsed and/or primary refractory HIV-associated NHL who were treated with pembrolizumab, an immune checkpoint inihibitor, with or without pomalidomide. Five patients had primary effusion lymphoma (PEL): one had germinal center B cell-like (GCB) diffuse large B cell lymphoma (DLBCL); two had non-GCB DLBCL; one had aggressive B cell lymphoma, not otherwise specified; and one had plasmablastic lymphoma. Six patients received pembrolizumab alone at 200 mg intravenously every 3 weeks, three received pembrolizumab 200 mg intravenously every 4 weeks plus pomalidomide 4 mg orally every day for days 1-21 of a 28-day cycle; and one sequentially received pembrolizumab alone and then pomalidomide alone. The response rate was 50% with particular benefit in gammaherpesvirus-associated tumors. The progression-free survival was 4.1 months (95% CI: 1.3 to 12.4) and overall survival was 14.7 months (95% CI: 2.96 to not reached). Three patients with PEL had leptomeningeal disease: one had a complete response and the other two had long-term disease control. There were four immune-related adverse events (irAEs), all CTCAEv5 grade 2-3; three of the four patients were able to continue receiving pembrolizumab. No irAEs occurred in patients receiving the combination of pembrolizumab and pomalidomide.
Conclusions: Treatment of HIV-associated NHL with pembrolizumab with or without pomalidomide elicited responses in several subtypes of HIV-associated NHL. This approach is worth further study in PLWH and NHL.
Keywords: hematologic neoplasms; immunomodulation; immunotherapy; programmed cell death 1 receptor.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Pembrolizumab for NCT02595866 was provided to the NCI by Merck and Co. KL, RR, TSU and RY report research funding through Cooperative Research and Development Agreements (CRADAs) between Celgene Corporation (now Bristol Myers Squibb, Co) and the National Cancer Institute as well as a CRADA between EMD-Serrono and the National Cancer Institute. RY has also used drugs for his clinical or laboratory research provided to the NCI by Genentech Corp, EMD-Serono, Janssen Research, and CTI Biopharma. RY and TSU are co-inventors on US Patent 10,001,483 entitled 'Methods for the treatment of Kaposi’s sarcoma or KSHV-induced lymphoma using immunomodulatory compounds, and uses of biomarkers'. The patent application for this was filed in part based on the results of NCI protocol 12-C-0047, entitled 'A Phase I/II Study of the Safety, Pharmacokinetics and Efficacy of Pomalidomide (CC-4047) in the Treatment of Kaposi Sarcoma in Individuals with or without HIV'. It is their understanding that foreign patents have also been filed for this invention. This invention was made as full-time employees of the US government under 45 Code of Federal Regulations Part 7. RY’s spouse, who is also a US Government employee, has a patent on KSHV viral IL-6. All rights, title, and interest to these patents have been or should by law be assigned to the US Department of Health and Human Services. The government conveys a portion of the royalties it receives to its employee-inventors under the Federal Technology Transfer Act of 1986 (PL 99-502). TSU reports research funding to Fred Hutchinson Cancer Center from Roche and consulting fees (<US$10,000) from AbbVie and Seattle Genetics. All other authors report no relevant conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources