

Characterisation of the T-cell response to Ebola virus glycoprotein amongst survivors of the 2013-16 West Africa epidemic
- PMID: 33608536
- PMCID: PMC7895930
- DOI: 10.1038/s41467-021-21411-0
Characterisation of the T-cell response to Ebola virus glycoprotein amongst survivors of the 2013-16 West Africa epidemic
Abstract
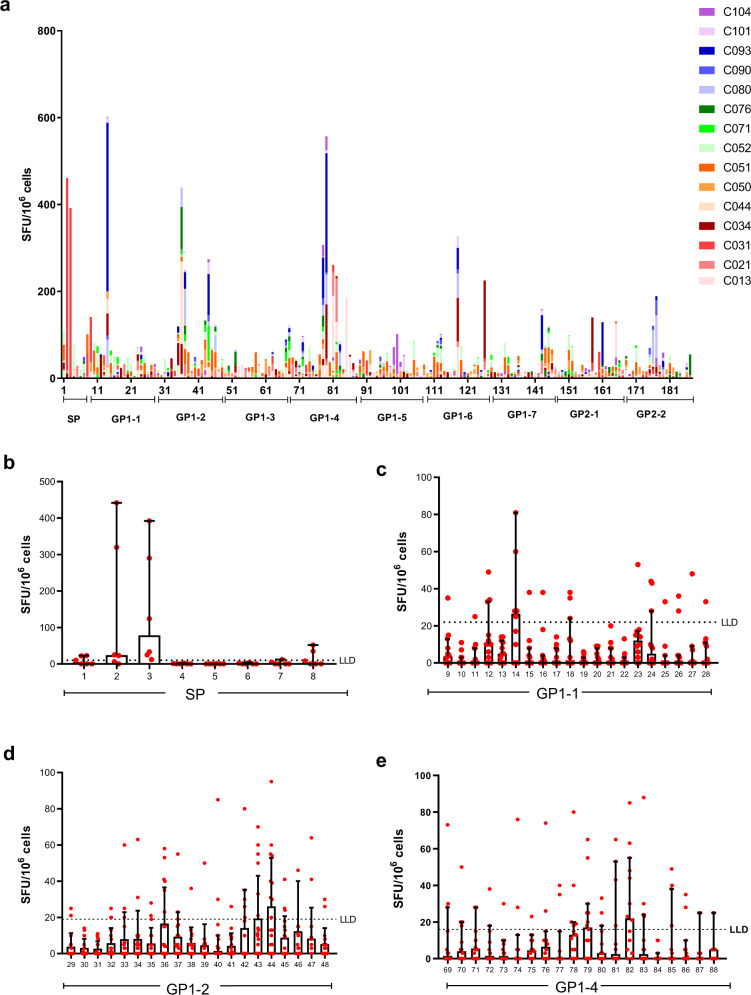
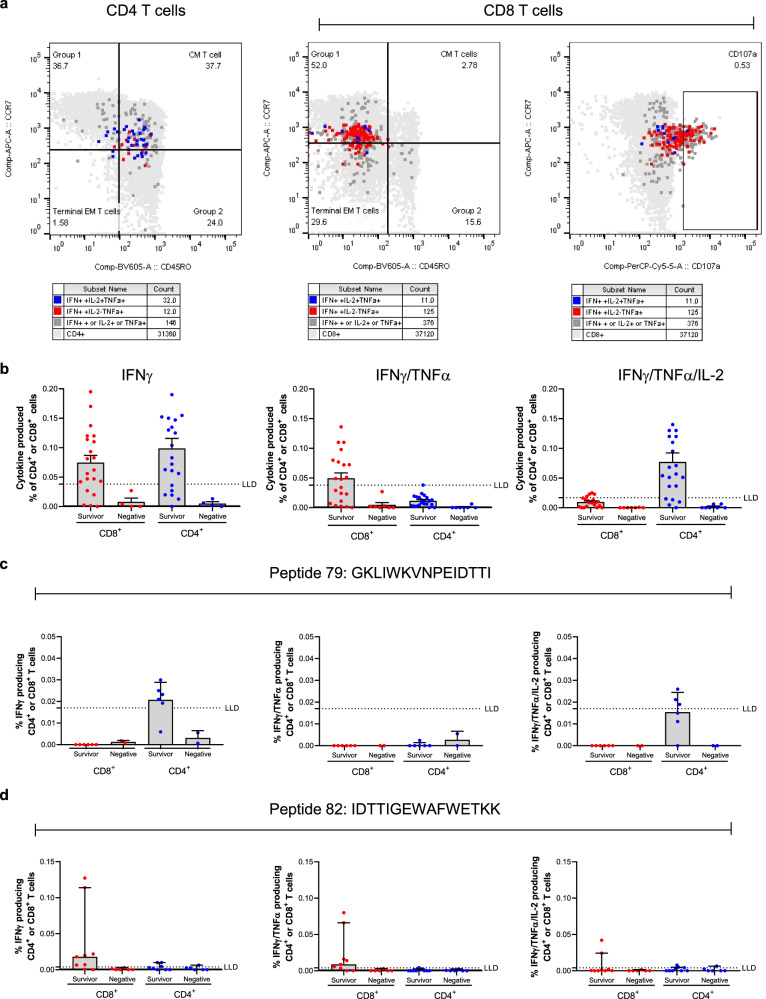
Zaire ebolavirus (EBOV) is a highly pathogenic filovirus which can result in Ebola virus disease (EVD); a serious medical condition that presents as flu like symptoms but then often leads to more serious or fatal outcomes. The 2013-16 West Africa epidemic saw an unparalleled number of cases. Here we show characterisation and identification of T cell epitopes in surviving patients from Guinea to the EBOV glycoprotein. We perform interferon gamma (IFNγ) ELISpot using a glycoprotein peptide library to identify T cell epitopes and determine the CD4+ or CD8+ T cell component response. Additionally, we generate data on the T cell phenotype and measure polyfunctional cytokine secretion by these antigen specific cells. We show candidate peptides able to elicit a T cell response in EBOV survivors and provide inferred human leukocyte antigen (HLA) allele restriction. This data informs on the long-term T cell response to Ebola virus disease and highlights potentially important immunodominant peptides.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
