

Quantifying pulmonary perfusion from noncontrast computed tomography
- PMID: 33608933
- PMCID: PMC8252085
- DOI: 10.1002/mp.14792
Quantifying pulmonary perfusion from noncontrast computed tomography
Abstract
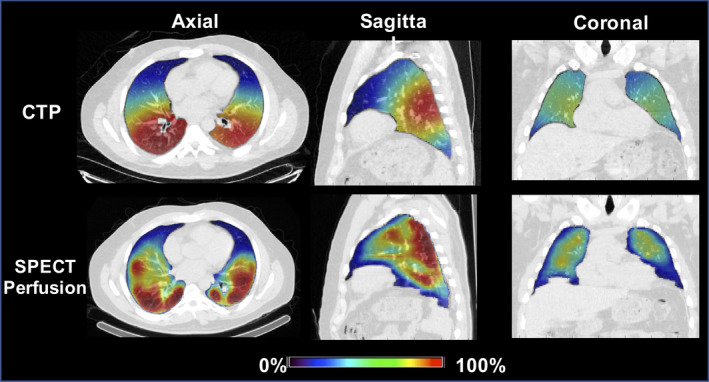
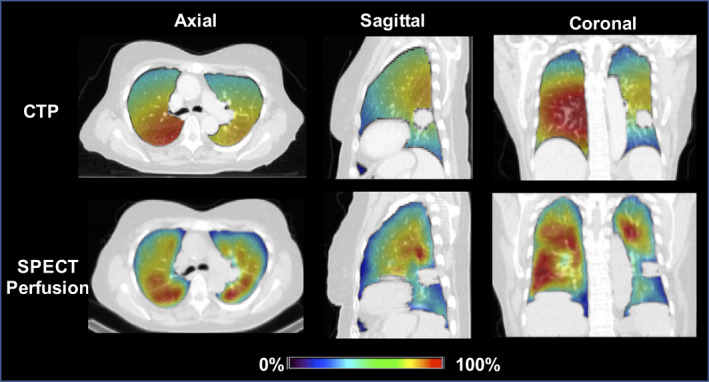
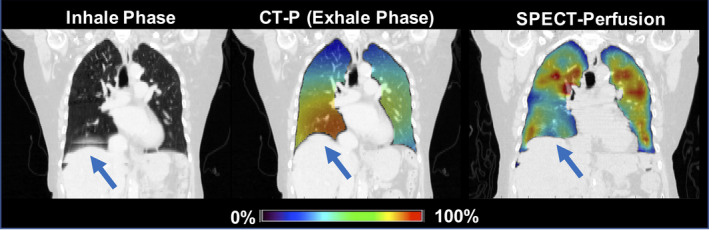
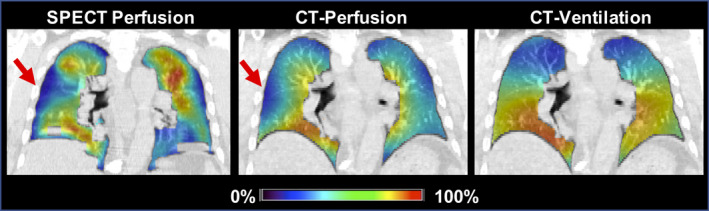
Purpose: Computed tomography (CT)-derived ventilation methods compute respiratory induced volume changes as a surrogate for pulmonary ventilation. Currently, there are no known methods to derive perfusion information from noncontrast CT. We introduce a novel CT-Perfusion (CT-P) method for computing the magnitude mass changes apparent on dynamic noncontrast CT as a surrogate for pulmonary perfusion.
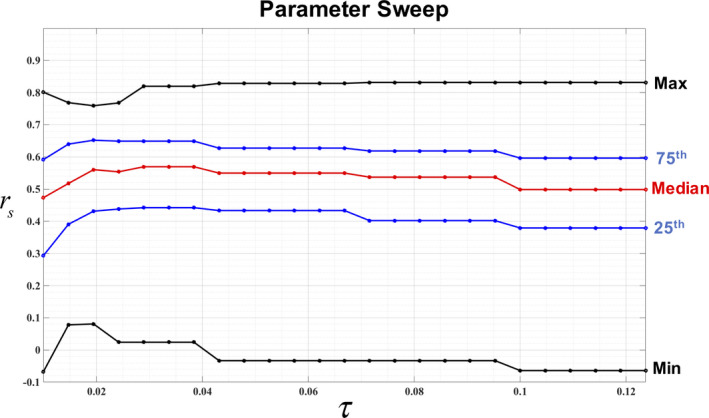
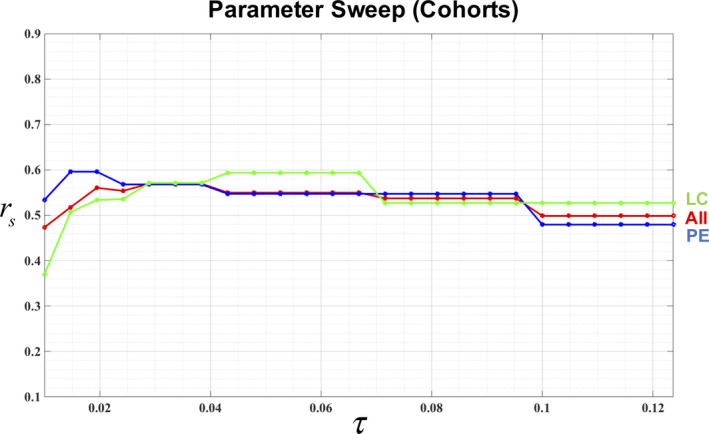
Methods: CT-Perfusion is based on a mass conservation model which describes the unknown mass change as a linear combination of spatially corresponding inhale and exhale HU estimated voxel densities. CT-P requires a deformable image registration (DIR) between the inhale/exhale lung CT pair, a preprocessing lung volume segmentation, and an estimate for the Jacobian of the DIR transformation. Given this information, the CT-P image, which provides the magnitude mass change for each voxel within the lung volume, is formulated as the solution to a constrained linear least squares problem defined by a series of subregional mean magnitude mass change measurements. Similar to previous robust CT-ventilation methods, the amount of uncertainty in a subregional sample mean measurement is related to measurement resolution and can be characterized with respect to a tolerance parameter . Spatial Spearman correlation between single photon emission CT perfusion (SPECT-P) and the proposed CT-P method was assessed in two patient cohorts via a parameter sweep of . The first cohort was comprised of 15 patients diagnosed with pulmonary embolism (PE) who had SPECT-P and 4DCT imaging acquired within 24 h of PE diagnosis. The second cohort was comprised of 15 nonsmall cell lung cancer patients who had SPECT-P and 4DCT images acquired prior to radiotherapy. For each test case, CT-P images were computed for 30 different uncertainty parameter values, uniformly sampled from the range [0.01, 0.125], and the Spearman correlation between the SPECT-P and the resulting CT-P images were computed.
Results: The median correlations between CT-P and SPECT-P taken over all 30 test cases ranged between 0.49 and 0.57 across the parameter sweep. For the optimal tolerance τ = 0.0385, the CT-P and SPECT-P correlations across all 30 test cases ranged between 0.02 and 0.82. A one-sample sign test was applied separately to the PE and lung cancer cohorts. A low Spearmen correlation of 15% was set as the null median value and two-sided alternative was tested. The PE patients showed a median correlation of 0.57 (IQR = 0.305). One-sample sign test was statistically significant with 96.5 % confidence interval: 0.20-0.63, P < 0.00001. Lung cancer patients had a median correlation of 0.57(IQR = 0.230). Again, a one-sample sign test for median was statistically significant with 96.5 percent confidence interval: 0.45-0.71, P < 0.00001.
Conclusion: CT-Perfusion is the first mechanistic model designed to quantify magnitude blood mass changes on noncontrast dynamic CT as a surrogate for pulmonary perfusion. While the reported correlations with SPECT-P are promising, further investigation is required to determine the optimal CT acquisition protocol and numerical method implementation for CT-P imaging.
Keywords: 4DCT; SPECT perfusion; computed tomography; deformable image registration; perfusion; ventilation.
© 2021 The Authors. Medical Physics published by Wiley Periodicals LLC on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no conflict to disclose.
Figures
References
-
- Guerrero T, Sanders K, Noyola‐Martinez J, et al. Quantification of regional ventilation from treatment planning CT. Intl J Radiat Oncol Biol Phys. 2005;62:630–634. - PubMed
-
- Castillo R, Castillo E, Martinez J, Guerrero T. Ventilation from four‐dimensional computed tomography: density versus Jacobian methods. Phys Med Biol. 2010;55:4661. - PubMed
-
- Yamamoto T, Kabus S, Bal M, Keall P, Benedict S, Daly M. The first patient treatment of computed tomography ventilation functional image‐guided radiotherapy for lung cancer. Radiother Oncol. 2016;118:227–231. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
