

Serum potassium and outcomes in heart failure with preserved ejection fraction: a post-hoc analysis of the PARAGON-HF trial
- PMID: 33609066
- PMCID: PMC11497244
- DOI: 10.1002/ejhf.2134
Serum potassium and outcomes in heart failure with preserved ejection fraction: a post-hoc analysis of the PARAGON-HF trial
Abstract
Aims: The relationship between serum potassium concentration and outcomes in patients with heart failure and preserved ejection fraction (HFpEF) is not well-established. The aim of this study was to explore the association between serum potassium and clinical outcomes in the PARAGON-HF trial in which 4822 patients with HFpEF were randomised to treatment with sacubitril/valsartan or valsartan.
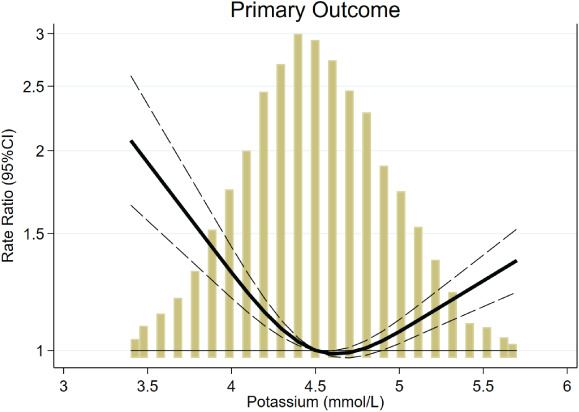
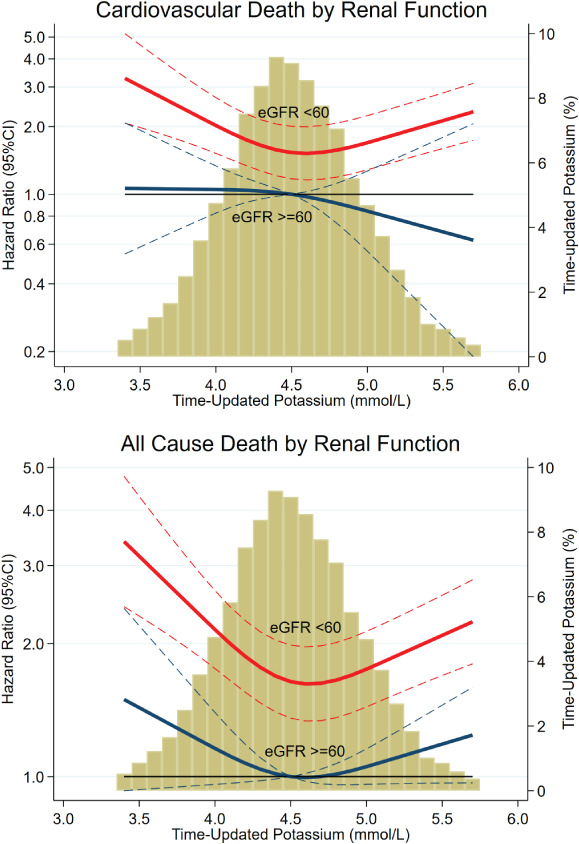
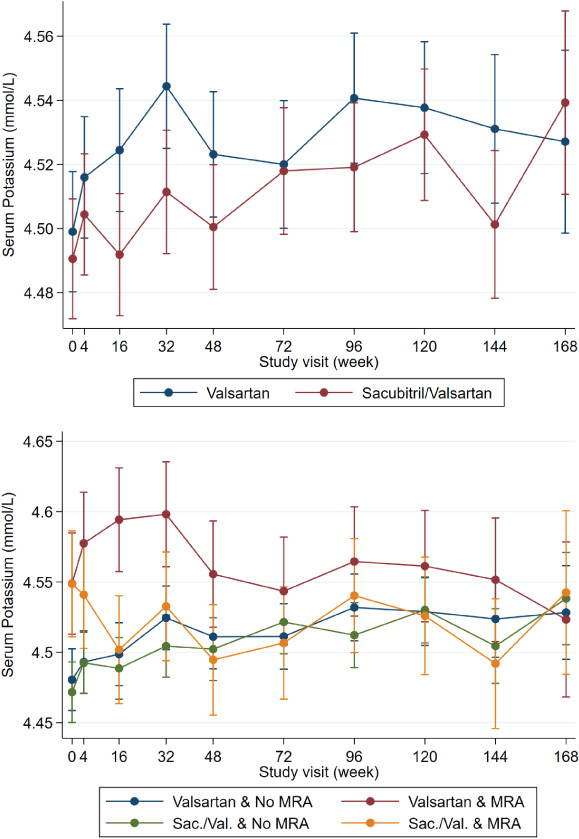
Methods and results: The relationship between serum potassium concentrations and the primary study composite outcome of total (first and recurrent) heart failure hospitalisations and cardiovascular death was analysed. Hypo-, normo-, and hyperkalaemia were defined as serum potassium <4 mmol/L, 4-5 mmol/L and >5 mmol/L, respectively. Both screening and time-updated potassium (categorical and continuous spline-transformed) were studied. Patient mean age was 73 years and 52% were women. Patients with higher baseline potassium more often had an ischaemic aetiology and diabetes and mineralocorticoid receptor antagonist treatment. Compared with normokalaemia, both time-updated (but not screening) hypo- and hyperkalaemia were associated with a higher risk of the primary outcome [adjusted hazard ratio (HR) for hypokalaemia 1.55, 95% confidence interval (CI) 1.30-1.85; P < 0.001, and for hyperkalaemia HR 1.21, 95% CI 1.02-1.44; P = 0.025]. Hypokalaemia had a stronger association with a higher risk of all-cause, cardiovascular and non-cardiovascular death than hyperkalaemia. The association of hypokalaemia with increased risk of all-cause and cardiovascular death was most marked in participants with impaired kidney function (interaction P < 0.05). Serum potassium did not significantly differ between sacubitril/valsartan and valsartan throughout the follow-up.
Conclusions: Both hypo- and hyperkalaemia were associated with heart failure hospitalisation but only hypokalaemia was associated with mortality, especially in the context of renal impairment. Hypokalaemia was as strongly associated with death from non-cardiovascular causes as with cardiovascular death. Collectively, these findings suggest that potassium disturbances are a more of a marker of HFpEF severity rather than a direct cause of death.
Keywords: Heart failure with preserved ejection fraction; Outcomes; Sacubitril/valsartan; Serum potassium.
© 2021 The Authors. European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures
References
-
- Savarese G, Xu H, Trevisan M, Dahlstrom U, Rossignol P, Pitt B, Lund LH, Carrero JJ. Incidence, predictors, and outcome associations of dyskalemia in heart failure with preserved, mid‐range, and reduced ejection fraction. JACC Heart Fail 2019;7:65–76. - PubMed
-
- Desai AS, Liu J, Pfeffer MA, Claggett B, Fleg J, Lewis EF, McKinlay S, O'Meara E, Shah SJ, Sweitzer NK, Solomon S, Pitt B. Incident hyperkalemia, hypokalemia, and clinical outcomes during spironolactone treatment of heart failure with preserved ejection fraction: analysis of the TOPCAT trial. J Card Fail 2018;24:313–320. - PubMed
-
- Nishihara T, Tokitsu T, Sueta D, Takae M, Oike F, Fujisue K, Usuku H, Takashio S, Hanatani S, Kanazawa H, Arima Y, Sakamoto K, Izumiya Y, Yamabe H, Kaikita K, Yamamoto E, Tsujita K. Serum potassium and cardiovascular events in heart failure with preserved left ventricular ejection fraction patients. Am J Hypertens 2018;31:1098–1105. - PubMed
-
- Badr Eslam R, Öztürk B, Panzer S, Qin H, Duca F, Binder C, Rettl R, Dachs TM, Alasti F, Vila G, Bonderman D. Low serum potassium levels and diabetes – an unfavorable combination in patients with heart failure and preserved ejection fraction. Int J Cardiol 2020;317:121–127. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
