

Systematic approach towards reliable estimation of abdominal aortic aneurysm size by ultrasound imaging and CT
- PMID: 33609372
- PMCID: PMC7893461
- DOI: 10.1093/bjsopen/zraa041
Systematic approach towards reliable estimation of abdominal aortic aneurysm size by ultrasound imaging and CT
Abstract
Background: The management of abdominal aortic aneurysm (AAA) is fully dictated by AAA size, but there are no uniform measurement guidelines, and systematic differences exist between ultrasound- and CT-based size estimation. The aim of this study was to devise a uniform ultrasound acquisition and measurement protocol, and to test whether harmonization of ultrasound and CT readings is feasible.
Methods: A literature review was undertaken to evaluate evidence for ultrasound-based measurement of AAA. A protocol for measuring AAA was then developed, and intraobserver and interobserver reproducibility was tested. Finally, agreement between ultrasound readings and CT-based AAA diameters was evaluated. This was an observational study of patients with a small AAA who participated in two pharmaceutical intervention trials.
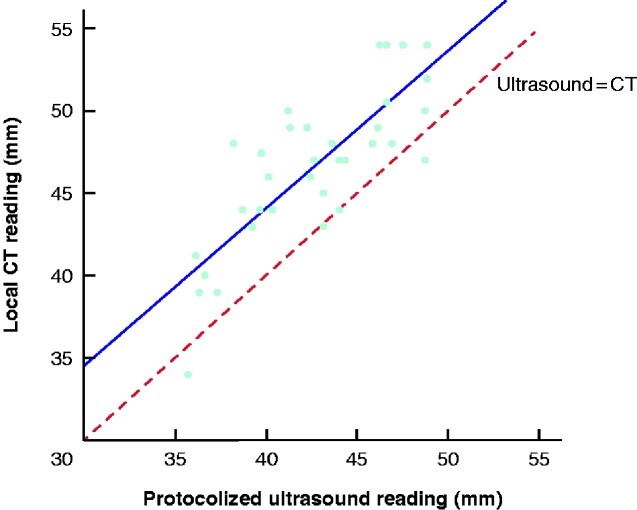
Results: Based on a literature review, an ultrasound acquisition and reading protocol was devised. Evaluation of the protocol showed an intraobserver repeatability of 1.6 mm (2s.d.) and an interobserver intraclass correlation coefficient (ICC) of 0.97. Comparison of protocolled ultrasound readings and local CT readings indicated a good correlation (r = 0.81), but a systematic +4.1-mm difference for CT. Harmonized size readings for ultrasound imaging and CT increased the correlation (r = 0.91) and reduced the systematic difference to +1.8 mm by CT. Interobserver reproducibility of protocolized CT measurements showed an ICC of 0.94 for the inner-to-inner method and 0.96 for the outer-to-outer method.
Conclusion: The absence of harmonized size acquisition and reading guidelines results in overtreatment and undertreatment of patients with AAA. This can be avoided by the implementation of standardized ultrasound acquisition and a harmonized reading protocol for ultrasound- and CT-based readings.
© The Author(s) 2021. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures



Similar articles
-
Variability in measurement of abdominal aortic aneurysms. Abdominal Aortic Aneurysm Detection and Management Veterans Administration Cooperative Study Group.J Vasc Surg. 1995 Jun;21(6):945-52. doi: 10.1016/s0741-5214(95)70222-9. J Vasc Surg. 1995. PMID: 7776474 Clinical Trial.
-
Three-dimensional ultrasound evaluation of small asymptomatic abdominal aortic aneurysms.Eur J Vasc Endovasc Surg. 2015 Mar;49(3):289-96. doi: 10.1016/j.ejvs.2014.12.022. Epub 2015 Feb 4. Eur J Vasc Endovasc Surg. 2015. PMID: 25662155
-
Automated software supported versus manual aorto-iliac diameter measurements in CT angiography of patients with abdominal aortic aneurysms: assessment of inter- and intraobserver variation.Vasa. 2005 Nov;34(4):255-61. doi: 10.1024/0301-1526.34.4.255. Vasa. 2005. PMID: 16363281
-
Reproducibility of ultrasound measurement of the abdominal aorta.Br J Surg. 2011 Nov;98(11):1517-25. doi: 10.1002/bjs.7628. Epub 2011 Aug 22. Br J Surg. 2011. PMID: 21861264 Review.
-
Measuring the maximum diameter of native abdominal aortic aneurysms: review and critical analysis.Eur J Vasc Endovasc Surg. 2012 May;43(5):515-24. doi: 10.1016/j.ejvs.2012.01.018. Epub 2012 Feb 14. Eur J Vasc Endovasc Surg. 2012. PMID: 22336051 Review.
Cited by
-
EVAR Follow-Up with Ultrasound Superb Microvascular Imaging (SMI) Compared to CEUS and CT Angiography for Detection of Type II Endoleak.Diagnostics (Basel). 2022 Feb 18;12(2):526. doi: 10.3390/diagnostics12020526. Diagnostics (Basel). 2022. PMID: 35204615 Free PMC article.
-
3D-Ultrasound Based Mechanical and Geometrical Analysis of Abdominal Aortic Aneurysms and Relationship to Growth.Ann Biomed Eng. 2023 Nov;51(11):2554-2565. doi: 10.1007/s10439-023-03301-2. Epub 2023 Jul 6. Ann Biomed Eng. 2023. PMID: 37410199 Free PMC article.
-
A histopathological classification scheme for abdominal aortic aneurysm disease.JVS Vasc Sci. 2021 Oct 7;2:260-273. doi: 10.1016/j.jvssci.2021.09.001. eCollection 2021. JVS Vasc Sci. 2021. PMID: 34825232 Free PMC article.
References
-
- Moll FL, Powell JT, Fraedrich G, Verzini F, Haulon S, Waltham M et al. Management of abdominal aortic aneurysms clinical practice guidelines of the European Society for Vascular Surgery. Eur J Vasc Endovasc Surg 2011;41(Suppl 1):S1–S58 - PubMed
-
- Wanhainen A, Verzini F, Van Herzeele I, Allaire E, Bown M, Cohnert T et al. Editor's Choice – European Society for Vascular Surgery (ESVS) 2019 clinical practice guidelines on the management of abdominal aorto-iliac artery aneurysms. Eur J Vasc Endovasc Surg 2019;57:8–93 - PubMed
-
- Chaikof EL, Dalman RL, Eskandari MK, Jackson BM, Lee WA, Mansour MA et al. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J Vasc Surg 2018;67:2–77.e2 - PubMed
-
- Tomee SM, Lijftogt N, Vahl A, Hamming JF, Lindeman JHN. A registry-based rationale for discrete intervention thresholds for open and endovascular elective abdominal aortic aneurysm repair in female patients. J Vasc Surg 2018;67:735–739 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
