

Risk of stroke in relation to degree of asymptomatic carotid stenosis: a population-based cohort study, systematic review, and meta-analysis
- PMID: 33609477
- PMCID: PMC7889579
- DOI: 10.1016/S1474-4422(20)30484-1
Risk of stroke in relation to degree of asymptomatic carotid stenosis: a population-based cohort study, systematic review, and meta-analysis
Erratum in
-
Correction to Lancet Neurol 2021; 20: 193-20.Lancet Neurol. 2021 May;20(5):e4. doi: 10.1016/S1474-4422(21)00076-4. Epub 2021 Mar 16. Lancet Neurol. 2021. PMID: 33740440 Free PMC article. No abstract available.
Abstract
Background: There is uncertainty around which patients with asymptomatic carotid stenosis should be offered surgical intervention. Although stroke rates were unrelated to the degree of stenosis in the medical-treatment-only groups in previous randomised trials, this could simply reflect recruitment bias and there has been no systematic analysis of a stenosis-risk association in cohort studies. We aimed to establish whether there is any association between the degree of asymptomatic stenosis and ipsilateral stroke risk in patients on contemporary medical treatment.
Methods: We did a prospective population-based study (Oxford Vascular Study; OxVasc), and a systematic review and meta-analysis. All patients in OxVasc with a recent suspected transient ischaemic attack or stroke, between April 1, 2002, and April 1, 2017, who had asymptomatic carotid stenosis were included in these analyses. We commenced contemporary medical treatment and determined ipsilateral stroke risk in this cohort by face-to-face follow-up (to Oct 1, 2020). We also did a systematic review and meta-analysis of all published studies (from Jan 1, 1980, to Oct 1, 2020) reporting ipsilateral stroke risk in patients with asymptomatic carotid stenosis. We searched MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials, and included both observational cohort studies and medical treatment groups of randomised controlled trials if the number of patients exceeded 30, ipsilateral stroke rates (or the raw data to calculate these) were provided, and were published in English.
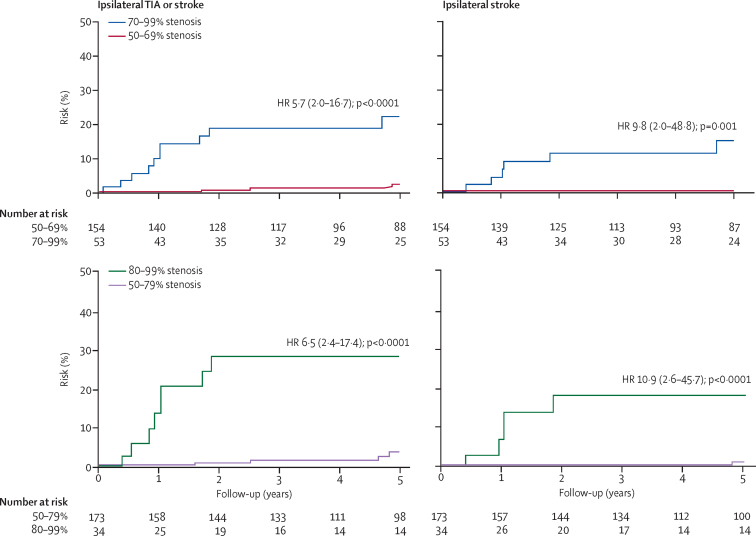
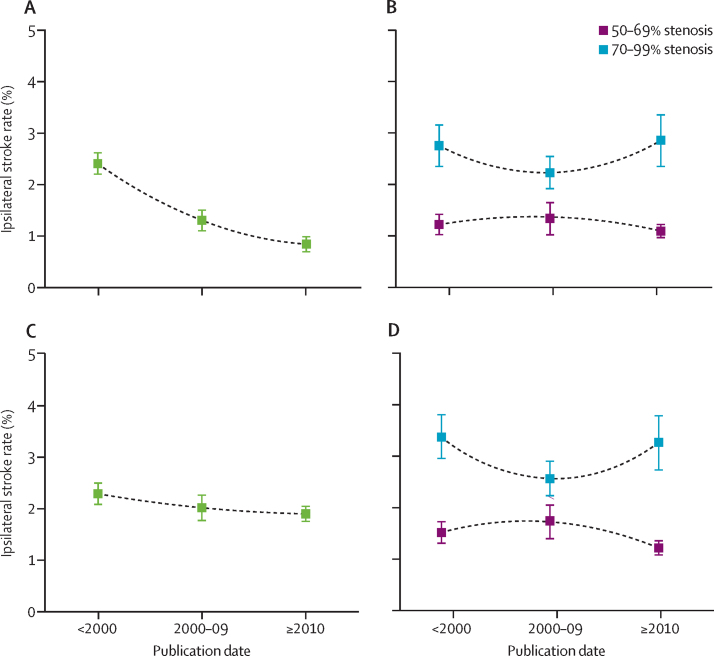
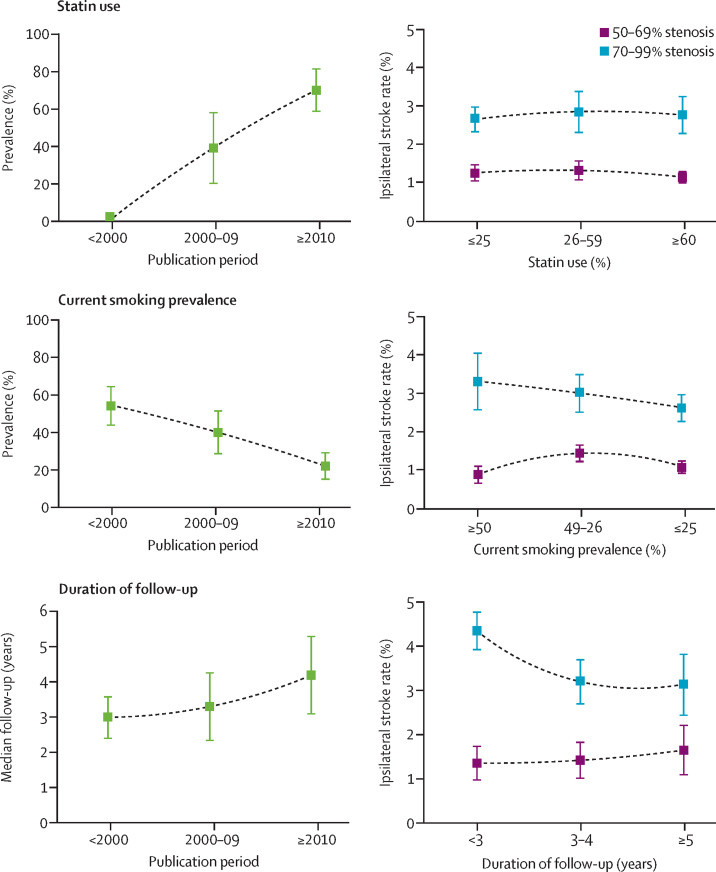
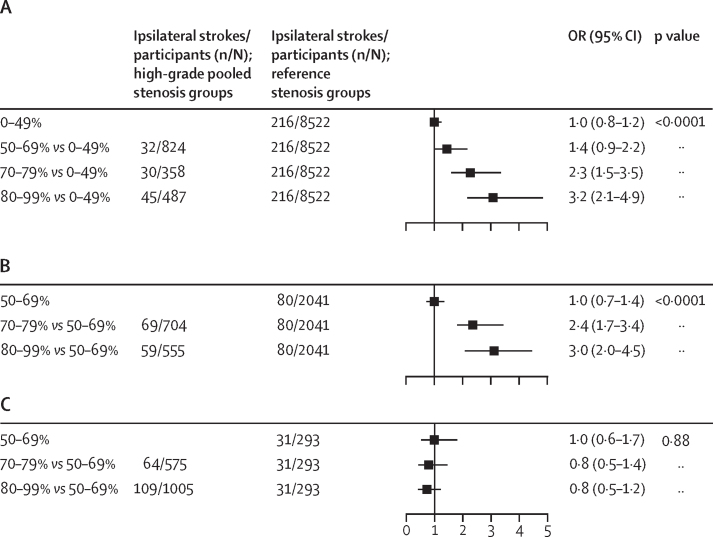
Findings: Between April 1, 2002, and April 1, 2017, 2354 patients were consecutively enrolled in OxVasc and 2178 patients underwent carotid imaging, of whom 207 had 50-99% asymptomatic stenosis of at least one carotid bifurcation (mean age at imaging: 77·5 years [SD 10·3]; 88 [43%] women). The 5-year ipsilateral stroke risk increased with the degree of stenosis; patients with 70-99% stenosis had a significantly greater 5-year ipsilateral stroke risk than did those with 50-69% stenosis (six [14·6%; 95% CI 3·5-25·7] of 53 patients vs none of 154; p<0·0001); and patients with 80-99% stenosis had a significantly greater 5-year ipsilateral stroke risk than did those with 50-79% stenosis (five [18·3%; 7·7-29·9] of 34 patients vs one [1·0%; 0·0-2·9] of 173; p<0·0001). Of the 56 studies identified in the systematic review (comprising 13 717 patients), 23 provided data on ipsilateral stroke risk fully stratified by degree of asymptomatic stenosis (in 8419 patients). Stroke risk was linearly associated with degree of ipsilateral stenosis (p<0·0001); there was a higher risk in patients with 70-99% stenosis than in those with 50-69% stenosis (386 of 3778 patients vs 181 of 3806 patients; odds ratio [OR] 2·1 [95% CI 1·7-2·5], p<0·0001; 15 cohort studies, three trials) and a higher risk in patients with 80-99% stenosis than in those with 50-79% stenosis (77 of 727 patients vs 167 of 3272 patients; OR 2·5 [1·8-3·5], p<0·0001; 11 cohort studies). Heterogeneity in stroke risk between studies for patients with severe versus moderate stenosis (phet<0·0001) was accounted for by highly discrepant results (pdiff<0·0001) in the randomised controlled trials of endarterectomy compared with cohort studies (trials: pooled OR 0·8 [95% CI 0·6-1·2], phet=0·89; cohorts: 2·9 [2·3-3·7], phet=0·54).
Interpretation: Contrary to the assumptions of current guidelines and the findings of subgroup analyses of previous randomised controlled trials, the stroke risk reported in cohort studies was highly dependent on the degree of asymptomatic carotid stenosis, suggesting that the benefit of endarterectomy might be underestimated in patients with severe stenosis. Conversely, the 5-year stroke risk was low for patients with moderate stenosis on contemporary medical treatment, calling into question any benefit from revascularisation.
Funding: NIHR Oxford Biomedical Research Centre, Wellcome Trust, Wolfson Foundation, and the British Heart Foundation.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Treatment of asymptomatic carotid stenosis.Lancet Neurol. 2021 Mar;20(3):163-165. doi: 10.1016/S1474-4422(21)00006-5. Lancet Neurol. 2021. PMID: 33609465 No abstract available.
References
-
- European Carotid Surgery Trialists' Collaborative Group Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST) Lancet. 1998;351:1379–1387. - PubMed
-
- Barnett HJM, Taylor DW, Haynes RB. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991;325:445–453. - PubMed
-
- Sacco RL, Adams R, Albers G. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Stroke. 2006;37:577–617. - PubMed
-
- NICE . National Institute for Health and Clinical Excellence; London: 2008. Diagnosis and initial management of acute stroke and transient ischaemic attack (TIA). CG38.
-
- Rothwell PM, Eliasziw M, Gutnikov SA. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361:107–116. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
