

Perineal reconstruction with pedicled rectus abdominis myocutaneous flap after posterior pelvic exenteration -A 3D model study
- PMID: 33609946
- PMCID: PMC7903330
- DOI: 10.1016/j.ijscr.2021.02.015
Perineal reconstruction with pedicled rectus abdominis myocutaneous flap after posterior pelvic exenteration -A 3D model study
Abstract
Introduction: Limited literature exists regarding the positional relationship between the pedicled-rectus abdominis myocutaneous (p-RAMC) flap and residual pelvic organs post posterior pelvic exenteration (PPE).
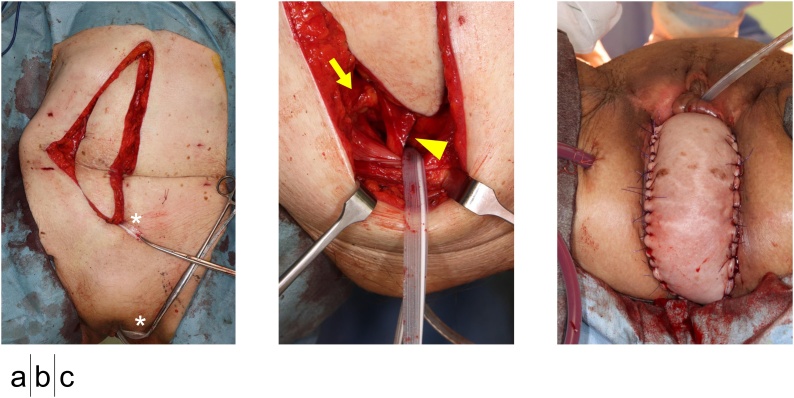
Presentation of case: Four patients underwent PPE and reconstruction with a p-RAMC flap. After harvesting the p-RAMC flap with the deep inferior epigastric artery and veins as the vascular pedicle, the intra-pelvic shortest pathway of the flap was created. We dissected the subcutaneous tissues of the flap donor site toward the perineal defect along the inner wall of the pelvis. The pubic origin of the rectus abdominis muscle was preserved. A three-dimensional model was constructed using an image processing software. The vascular pedicle ran almost linearly along the inner wall of the pelvis. The muscle belly was placed on the pelvic floor through the posterior wall of the urinary bladder which filled the dead space of the resected area. All flaps survived without significant complications.
Discussion: Assigning the cranial side of the flap to the perineum and caudal side to the pelvic floor could reduce postoperative intrapelvic complications. By preserving the pubic origin of the rectus abdominis muscle, a shock absorber of the pedicle of the flap was created, preventing over-traction of the flap while passing through the intrapelvic pathway.
Conclusion: A p-RAMC flap via intra-pelvic shortest pathway is an ideal reconstructive method for large skin defect in perineal area after PPE.
Keywords: Case-Series; Computed tomography; Pedicled-Rectus abdominis myocutaneous flap; Perineal reconstruction; Three-Dimensional model.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures



References
-
- Loughrey M.B., McManus D.T. Springer; 2004. Pelvic Exenteration Specimens. Histopathology Specimens; pp. 351–355.
-
- Nelson R.A., Butler C.E. Surgical outcomes of VRAM versus thigh flaps for immediate reconstruction of pelvic and perineal cancer resection defects. Plast. Reconstr. Surg. 2009;123:175–183. - PubMed
-
- Miyamoto Y., Akiyama T., Sakamoto Y., Tokunaga R., Ohuchi M., Shigaki H. Omental flap after pelvic exenteration for pelvic cancer. Surg. Today. 2016;46:1471–1475. - PubMed
-
- Agha R.A., Borreli M.R., Farwana R., Koshy K., Fowler A., Orgill D.P. The SCARE 2018 statement: Updating consensus Surgical CAse REport (SCARE) guidelines. Int. J. Surg. 2018;60:132–136. - PubMed
-
- Tobin G.R., Day T.G. Vaginal and pelvic reconstruction with distally based rectus abdominis myocutaneous flaps. Plast. Reconstr. Surg. 1988;18:62–70. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
