

Cediranib in addition to chemotherapy for women with relapsed platinum-sensitive ovarian cancer (ICON6): overall survival results of a phase III randomised trial
- PMID: 33610123
- PMCID: PMC7903311
- DOI: 10.1016/j.esmoop.2020.100043
Cediranib in addition to chemotherapy for women with relapsed platinum-sensitive ovarian cancer (ICON6): overall survival results of a phase III randomised trial
Abstract
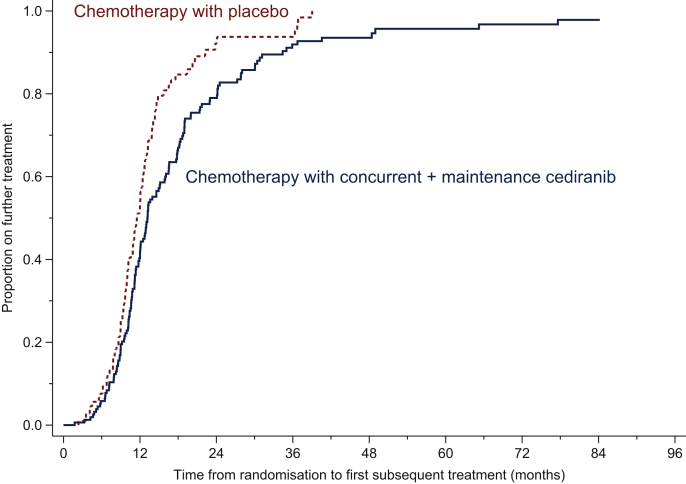
Background: Cediranib, an oral anti-angiogenic VEGFR 1-3 inhibitor, was studied at a daily dose of 20 mg in combination with platinum-based chemotherapy and as maintenance in a randomised trial in patients with first relapse of 'platinum-sensitive' ovarian cancer and has been shown to improve progression-free survival (PFS).
Patients and methods: ICON6 (NCT00532194) was an international three-arm, double-blind, placebo-controlled randomised trial. Between December 2007 and December 2011, 456 women were randomised, using stratification, to receive either chemotherapy with placebo throughout (arm A, reference); chemotherapy with concurrent cediranib, followed by maintenance placebo (arm B, concurrent); or chemotherapy with concurrent cediranib, followed by maintenance cediranib (arm C, maintenance). Due to an enforced redesign of the trial in September 2011, the primary endpoint became PFS between arms A and C which we have previously published, and the overall survival (OS) was defined as a secondary endpoint, which is reported here.
Results: After a median follow-up of 25.6 months, strong evidence of an effect of concurrent plus maintenance cediranib on PFS was observed [hazard ratio (HR) 0.56, 95% confidence interval (CI) 0.44-0.72, P < 0.0001]. In this final update of the survival analysis, 90% of patients have died. There was a 7.4-month difference in median survival and an HR of 0.86 (95% CI: 0.67-1.11, P = 0.24) in favour of arm C. There was strong evidence of a departure from the assumption of non-proportionality using the Grambsch-Therneau test (P = 0.0031), making the HR difficult to interpret. Consequently, the restricted mean survival time (RMST) was used and the estimated difference over 6 years by the RMST was 4.8 months (95% CI: -0.09 to 9.74 months).
Conclusions: Although a statistically significant difference in time to progression was seen, the enforced curtailment in recruitment meant that the secondary analysis of OS was underpowered. The relative reduction in the risk of death of 14% risk of death was not conventionally statistically significant, but this improvement and the increase in the mean survival time in this analysis suggest that cediranib may have worthwhile activity in the treatment of recurrent ovarian cancer and that further research should be undertaken.
Keywords: clinical trial; oncology; ovarian; overall survival; phase III.
Copyright © 2021. Published by Elsevier Ltd.
Conflict of interest statement
Disclosure ACE-T, HH, MV, ED, BP, LF, and AMS declare no conflicts of interest. JAL has attended AstraZeneca, GSK, Clovis Oncology, MSD, Eisai, Pfizer advisory boards and spoken at symposia with remuneration and has institutional grants from AstraZeneca and MSD. TJP reports grants, personal fees, non-financial support from Roche; personal fees from Novartis; personal fees from AstraZeneca, other fees paid to the institution from multiple other pharmaceutical companies and research organisations in connection with the costs of running a broad research portfolio, outside the submitted work. GCJ attended AstraZeneca advisory board and has received research funding for investigator-led trials. Also research grant from Roche. GJSR has attended advisory boards for AstraZeneca, Amgen and OXiGENE, in addition to data management costs from the MRC. SBK has attended an AstraZeneca advisory board. AO is Principal Investigator for investigator-initiated trials with AstraZeneca and has institutional grants from AstraZeneca outside the submitted work, and non compensated membership of steering committees with AstraZeneca and Clovis and a noncompensated advisory role with AstraZeneca and GSK. MF has attended advisory board meetings for AstraZeneca, Takeda, Novartis, MSD and Lilly and received personal fees. Travel support from AstraZeneca, research funding to institution for investigator-initiated trials. AG-M reports personal fees for advisory boards to Amgen, AstraZeneca, Clovis, Genmab, GSK-TESARO, Novartis, MSD, Oncoinvent, PharmaMar, Pfizer-Merck, Roche, SOTIO. RSK reports grants from Cancer Research UK and AstraZeneca, as well as drug supply from AstraZeneca. MKBP reports an educational grant from AstraZeneca.
Figures


References
-
- Jayson G.C., Kohn E.C., Kitchener H.C., Ledermann J.A. Ovarian cancer. Lancet. 2014;384:1376–1388. - PubMed
-
- Hicklin D.J., Ellis L.M. Role of the vascular endothelial growth factor pathway in tumor growth and angiogenesis. J Clin Oncol. 2005;23:1011–1027. - PubMed
-
- Perren T.J., Swart A.M., Pfisterer J. A phase 3 trial of bevacizumab in ovarian cancer. N Engl J Med. 2011;365:2484–2496. - PubMed
-
- Aghajanian C., Blank S.V., Goff B.A. OCEANS: a randomized, double-blind, placebo-controlled phase III trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube cancer. J Clin Oncol. 2012;30:2039–2045. - PMC - PubMed
-
- Pujade-Lauraine E., Hilpert F., Weber B. Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: the AURELIA open-label randomized phase III trial. J Clin Oncol. 2014;32:1302–1308. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
