

Immune profiling of Mycobacterium tuberculosis-specific T cells in recent and remote infection
- PMID: 33610126
- PMCID: PMC7902886
- DOI: 10.1016/j.ebiom.2021.103233
Immune profiling of Mycobacterium tuberculosis-specific T cells in recent and remote infection
Abstract
Background: Recent Mycobacterium tuberculosis (M.tb) infection is associated with a higher risk of progression to tuberculosis disease, compared to persistent infection after remote exposure. However, current immunodiagnostic tools fail to distinguish between recent and remote infection. We aimed to characterise the immunobiology associated with acquisition of M.tb infection and identify a biomarker that can distinguish recent from remote infection.
Methods: Healthy South African adolescents were serially tested with QuantiFERON-TB Gold to define recent (QuantiFERON-TB conversion <6 months) and persistent (QuantiFERON-TB+ for >1.5 year) infection. We characterised M.tb-specific CD4 T cell functional (IFN-γ, TNF, IL-2, CD107, CD154), memory (CD45RA, CCR7, CD27, KLRG-1) and activation (HLA-DR) profiles by flow cytometry after CFP-10/ESAT-6 peptide pool or M.tb lysate stimulation. We then assessed the diagnostic performance of immune profiles that were differentially expressed between individuals with recent or persistent QuantiFERON-TB+.
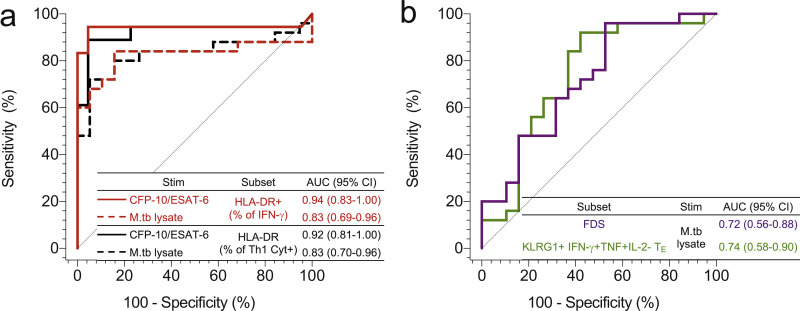
Findings: CFP-10/ESAT-6-specific CD4 T cell activation but not functional or memory phenotypes distinguished between individuals with recent and persistent QuantiFERON-TB+. In response to M.tb lysate, recent QuantiFERON-TB+ individuals had lower proportions of highly differentiated IFN-γ+TNF+ CD4 T cells expressing a KLRG-1+ effector phenotype and higher proportions of early differentiated IFN-γ-TNF+IL-2+ and activated CD4 T cells compared to persistent QuantiFERON-TB+ individuals. Among all differentially expressed T cell features CFP-10/ESAT-6-specific CD4 T cell activation was the best performing diagnostic biomarker of recent infection.
Interpretation: Recent M.tb infection is associated with highly activated and moderately differentiated functional M.tb-specific T cell subsets, that can be used as biomarkers to distinguish between recent and remote infection.
Funding: US National Institutes of Health (NIH), Bill and Melinda Gates Foundation, South African National Research Foundation, South African Medical Research Council, and Aeras.
Keywords: Biomarker; Recent infection; T cell activation; T cell differentiation; Tuberculosis.
Copyright © 2021 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Interests EN reports grants to the University of Cape Town from AERAS, Bill & Melinda Gates Foundation and NIH during the conduct of the study. TJS reports grants to the University of Cape Town from AERAS, Bill & Melinda Gates Foundation, and NIH during the conduct of the study. All other authors declare no competing interests.
Figures





References
-
- World Health Organisation. Global tuberculosis report 2020. Licence: CC BY-NC-SA 3.0 IGO. Available from: https://www.who.int/tb/publications/global_report/en/ (Accessed October 15 2020).
-
- Morán-Mendoza O, Marion SA, Elwood K, Patrick D, FitzGerald JM. Risk factors for developing tuberculosis: a 12-year follow-up of contacts of tuberculosis cases. Int J Tuberc Lung Dis Off J Int Union Against Tuberc Lung Dis. 2010;14:1112–1119. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
