

Pemafibrate decreases triglycerides and small, dense LDL, but increases LDL-C depending on baseline triglycerides and LDL-C in type 2 diabetes patients with hypertriglyceridemia: an observational study
- PMID: 33610176
- PMCID: PMC7897372
- DOI: 10.1186/s12944-021-01434-8
Pemafibrate decreases triglycerides and small, dense LDL, but increases LDL-C depending on baseline triglycerides and LDL-C in type 2 diabetes patients with hypertriglyceridemia: an observational study
Abstract
Background: Pemafibrate, a selective PPARα modulator, has the beneficial effects on serum triglycerides (TGs) and very low density lipoprotein (VLDL), especially in patients with diabetes mellitus or metabolic syndrome. However, its effect on the low density lipoprotein cholesterol (LDL-C) levels is still undefined. LDL-C increased in some cases together with a decrease in TGs, and the profile of lipids, especially LDL-C, during pemafibrate administration was evaluated.
Methods: Pemafibrate was administered to type 2 diabetes patients with hypertriglyceridemia. Fifty-one type 2 diabetes patients (mean age 62 ± 13 years) with a high rate of hypertension and no renal insufficiency were analyzed. Pemafibrate 0.2 mg (0.1 mg twice daily) was administered, and serum lipids were monitored every 4-8 weeks from 8 weeks before administration to 24 weeks after administration. LDL-C was measured by the direct method. Lipoprotein fractions were measured by electrophoresis (polyacrylamide gel, PAG), and LDL-migration index (LDL-MI) was calculated to estimate small, dense LDL.
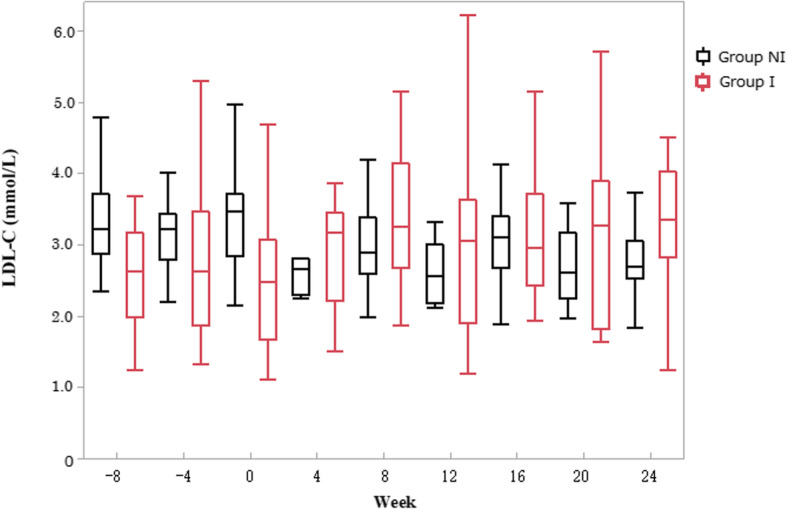
Results: Pemafibrate reduced serum TGs, midband and VLDL fractions by PAG. Pemafibrate increased LDL-C levels from baseline by 5.3% (- 3.8-19.1, IQR). Patients were divided into 2 groups: LDL-C increase of > 5.3% (group I, n = 25) and < 5.3% (group NI, n = 26) after pemafibrate. Compared to group NI, group I had lower LDL-C (2.53 [1.96-3.26] vs. 3.36 [3.05-3.72] mmol/L, P = 0.0009), higher TGs (3.71 [2.62-6.69] vs. 3.25 [2.64-3.80] mmol/L), lower LDL by PAG (34.2 [14.5, SD] vs. 46.4% [6.5], P = 0.0011), higher VLDL by PAG (28.2 [10.8] vs. 22.0% [5.2], P = 0.0234), and higher LDL-MI (0.421 [0.391-0.450] vs. 0.354 [0.341-0.396], P < 0.0001) at baseline. Pemafibrate decreased LDL-MI in group I, and the differences between the groups disappeared. These results showed contradictory effects of pemafibrate on LDL-C levels, and these effects were dependent on the baseline levels of LDL-C and TGs.
Conclusions: Pemafibrate significantly reduced TGs, VLDL, midband, and small, dense LDL, but increased LDL-C in diabetes patients with higher baseline TGs and lower baseline LDL-C. Even if pre-dose LDL-C remains in the normal range, pemafibrate improves LDL composition and may reduce cardiovascular disease risk.
Keywords: Dense LDL; Low density lipoprotein cholesterol; Pemafibrate; Small; Triglycerides; Type 2 daibetes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Cholesterol Treatment Trialistsʼ (CTT) Collaborators. Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380:581–590. doi: 10.1016/S0140-6736(12)60367-5. - DOI - PMC - PubMed
-
- Keech A, Simes RJ, Barter P, Best J, Scott R, Taskinen MR, et al. FIELD study investigators. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005;366:1849–1861. doi: 10.1016/S0140-6736(05)67667-2. - DOI - PubMed
-
- Cholesterol Treatment Trialists’ (CTT) Collaboration. Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681. doi: 10.1016/S0140-6736(10)61350-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
