

A multidisciplinary view of mastectomy and breast reconstruction: Understanding the challenges
- PMID: 33610903
- PMCID: PMC7905468
- DOI: 10.1016/j.breast.2021.02.004
A multidisciplinary view of mastectomy and breast reconstruction: Understanding the challenges
Abstract
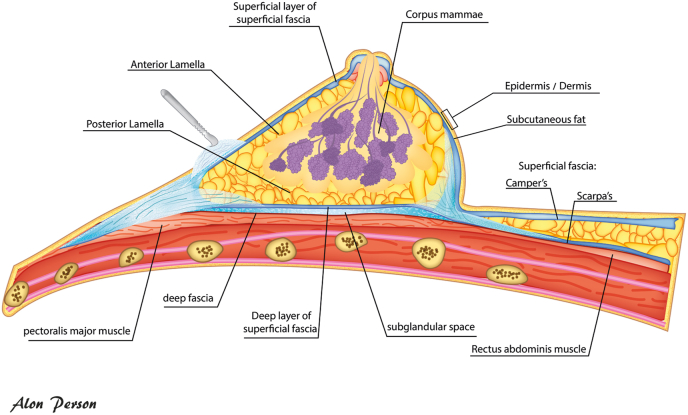
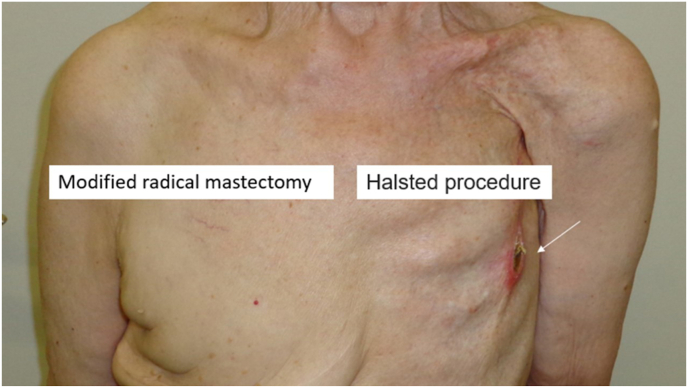
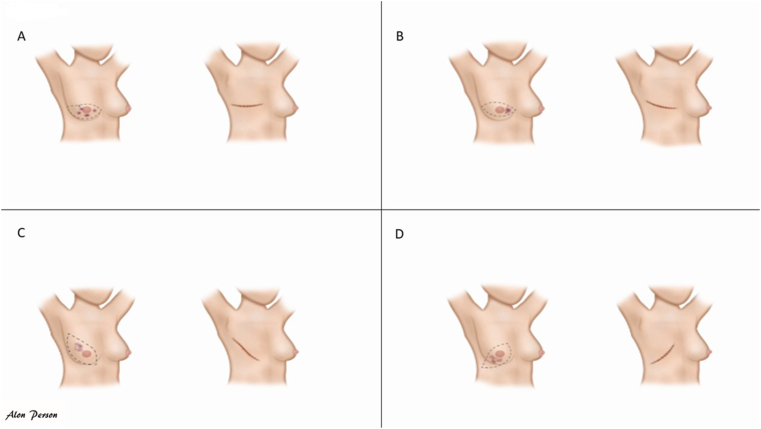
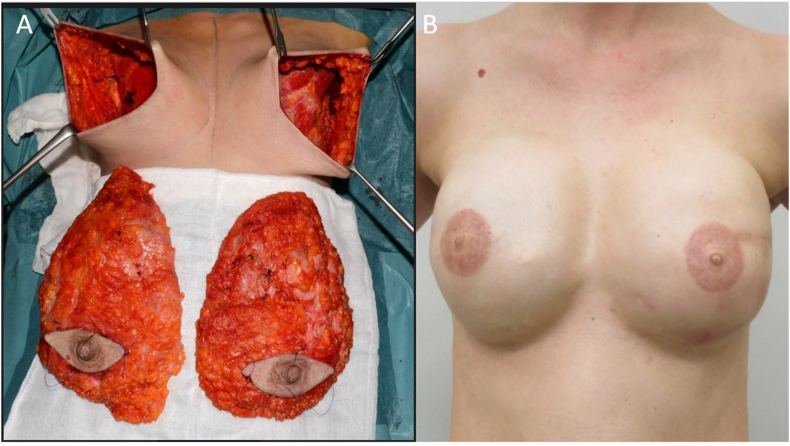
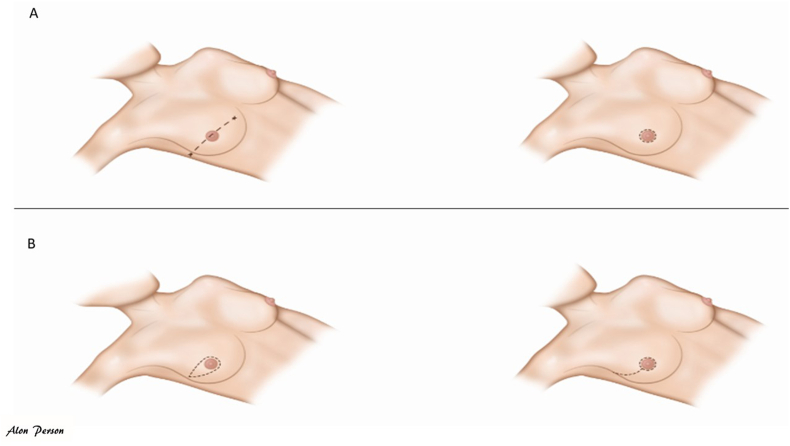
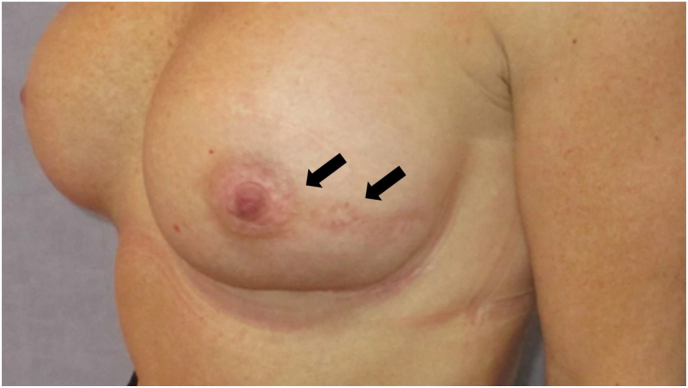
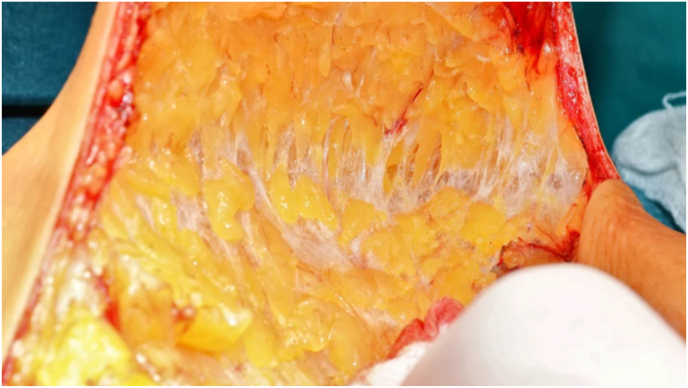
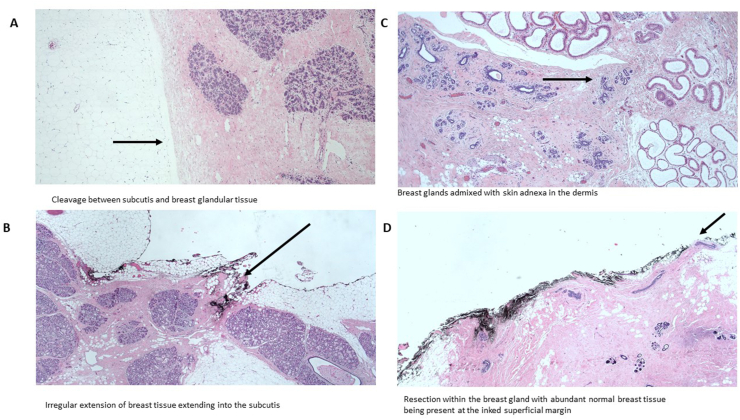
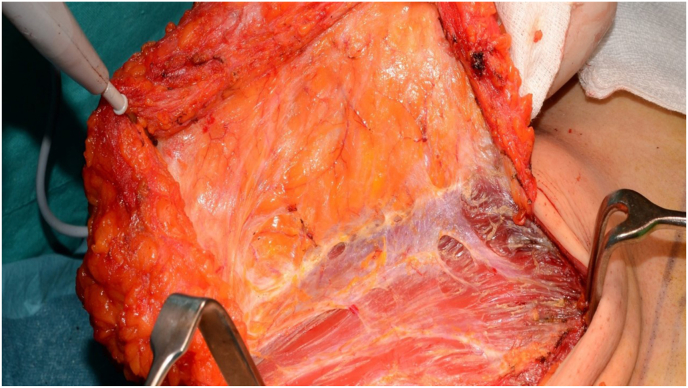
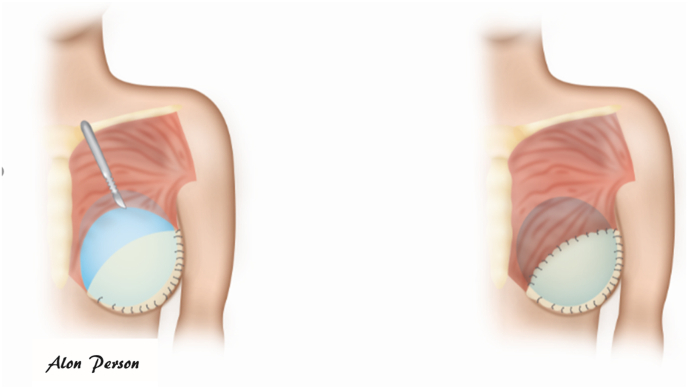
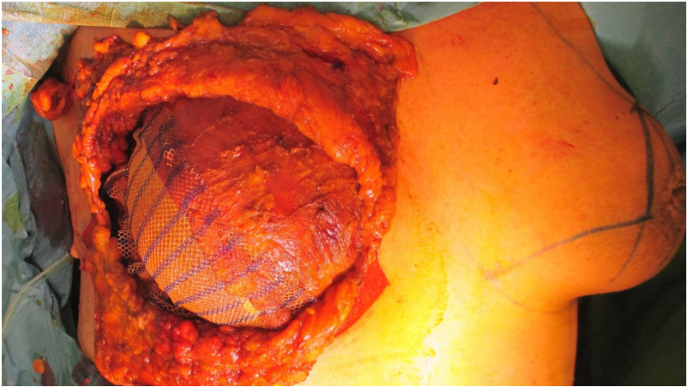
The current review paper was written in collaboration with breast cancer surgeons from the European Breast Cancer Research Association of Surgical Trialists (EUBREAST), a breast pathologist from the Danish Breast Cancer Group (DBCG), and representatives from the European SocieTy for Radiotherapy & Oncology (ESTRO) breast cancer course. Herein we summarize the different mastectomies and reconstruction procedures and define high-risk anatomical areas for breast cancer recurrences, to further specify the challenges in the surgical procedure, histopathological evaluation, and target volumes in case of postmastectomy irradiation, as recommended by the ESTRO guidelines according to the surgical procedure. The paper has original figures and illustrations for all disciplines for in-depth understanding of the differences between the procedures.
Keywords: Breast cancer; Mastectomy; Nipple sparing; Radiation; Reconstruction; Skin sparing.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest None relevant for the contents of this paper.
Figures

Similar articles
-
Nipple skin-sparing mastectomy is feasible for advanced disease.Ann Surg Oncol. 2013 Oct;20(10):3294-302. doi: 10.1245/s10434-013-3174-4. Epub 2013 Aug 22. Ann Surg Oncol. 2013. PMID: 23975304
-
Oncologic outcomes and radiation safety of nipple-sparing mastectomy with intraoperative radiotherapy for breast cancer.Breast Cancer. 2019 Sep;26(5):618-627. doi: 10.1007/s12282-019-00962-7. Epub 2019 Mar 19. Breast Cancer. 2019. PMID: 30888580
-
Favorable Outcome with Close Margins in Patients Undergoing Nipple/Skin Sparing Mastectomy with Immediate Breast Reconstruction: 5-year Follow-up.Balkan Med J. 2018 Jan 20;35(1):84-92. doi: 10.4274/balkanmedj.2017.0029. Epub 2017 Sep 29. Balkan Med J. 2018. PMID: 28958980 Free PMC article.
-
Nipple-sparing mastectomy: A review of outcomes at a single institution.Breast J. 2020 Nov;26(11):2183-2187. doi: 10.1111/tbj.14088. Epub 2020 Nov 2. Breast J. 2020. PMID: 33137841 Review.
-
Nipple-Sparing Mastectomy and Direct-to-Implant Breast Reconstruction.Plast Reconstr Surg. 2017 Nov;140(5S Advances in Breast Reconstruction):44S-50S. doi: 10.1097/PRS.0000000000003949. Plast Reconstr Surg. 2017. PMID: 29064921 Review.
Cited by
-
Comparison of the Preoperative MRI Evaluation of Glandular Tissue in Subcutaneous Mastectomy and its Influence on the Implant Volume.Cancer Diagn Progn. 2024 Sep 1;4(5):599-604. doi: 10.21873/cdp.10369. eCollection 2024 Sep-Oct. Cancer Diagn Progn. 2024. PMID: 39238620 Free PMC article.
-
Breast Radiotherapy after Oncoplastic Surgery-A Multidisciplinary Approach.Cancers (Basel). 2022 Mar 25;14(7):1685. doi: 10.3390/cancers14071685. Cancers (Basel). 2022. PMID: 35406457 Free PMC article. Review.
-
"How can a woman live without having a breast?": challenges related to mastectomy in Ethiopia.BMC Cancer. 2024 Jan 11;24(1):60. doi: 10.1186/s12885-023-11801-6. BMC Cancer. 2024. PMID: 38212706 Free PMC article.
-
Improved Survival after Breast-Conserving Therapy Compared with Mastectomy in Stage I-IIA Breast Cancer.Cancers (Basel). 2021 Aug 11;13(16):4044. doi: 10.3390/cancers13164044. Cancers (Basel). 2021. PMID: 34439197 Free PMC article.
-
Bilateral prophylactic mastectomy: should we preserve the pectoral fascia? Protocol of a Dutch double blinded, prospective, randomised controlled pilot study with a within-subject design (PROFAS).BMJ Open. 2023 Feb 17;13(2):e066728. doi: 10.1136/bmjopen-2022-066728. BMJ Open. 2023. PMID: 36806067 Free PMC article.
References
-
- Offersen B.V., Boersma L.J., Kirkove C. ESTRO consensus guideline on target volume delineation for elective radiation therapy of early stage breast cancer, version 1.1. Radiother Oncol. 2016;118:205–208. - PubMed
-
- Marks L.B., Kaidar-Person O., Poortmans P. Regarding current recommendations for postmastectomy radiation therapy in patients with one to three positive axillary lymph nodes. J Clin Oncol. 2017 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
