

Glomerular Filtration Rate in Asphyxiated Neonates Under Therapeutic Whole-Body Hypothermia, Quantified by Mannitol Clearance
- PMID: 33611729
- PMCID: PMC8249265
- DOI: 10.1007/s40262-021-00991-6
Glomerular Filtration Rate in Asphyxiated Neonates Under Therapeutic Whole-Body Hypothermia, Quantified by Mannitol Clearance
Abstract
Background: Therapeutic hypothermia (TH) is an established intervention to improve the outcome of neonates with moderate-to-severe hypoxic-ischemic encephalopathy resulting from perinatal asphyxia. Despite this beneficial effect, TH may further affect drug elimination pathways such as the glomerular filtration rate.
Objectives: The objective of this study was to quantify the effect of TH in addition to asphyxia on mannitol clearance as a surrogate for the glomerular filtration rate.
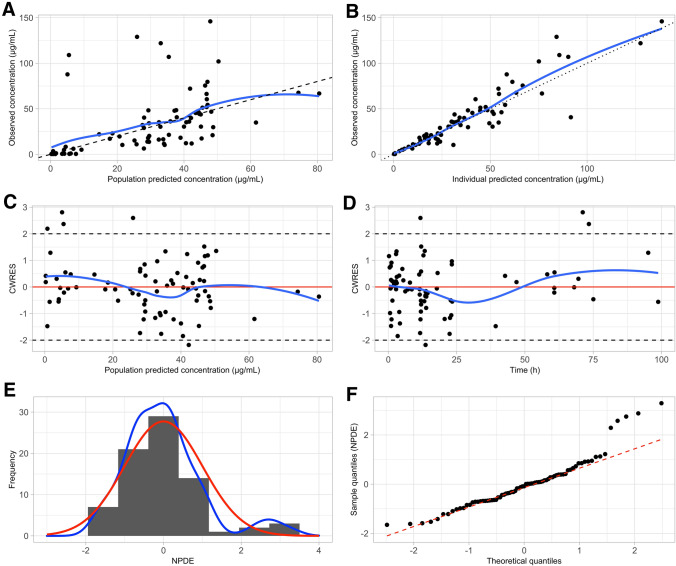
Methods: The effect of asphyxia and TH (mild vs moderate/severe) on mannitol clearance was assessed using a population approach, based on mannitol observations collected in the ALBINO (ALlopurinol in addition to TH for hypoxic-ischemic Brain Injury on Neurocognitive Outcome) trial, as some were exposed to a second dose of 10 mg/kg intravenous mannitol as placebo to ensure blinding. Pharmacokinetic analysis and model development were conducted using NONMEM version 7.4.
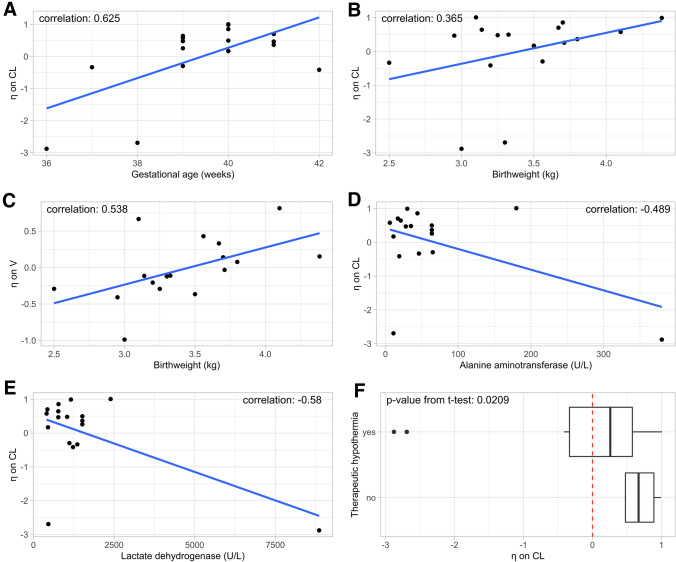
Results: Based on 77 observations from 17 neonates (TH = 13), a one-compartment model with first-order linear elimination best described the observed data. To account for prenatal glomerular filtration rate maturation, both birthweight and gestational age were implemented as clearance covariates using an earlier published three-quarters power function and a sigmoid hyperbolic function. Our final model predicted a mannitol clearance of 0.15 L/h for a typical asphyxia neonate (39.5 weeks, birthweight 3.25 kg, no TH), lower than the reported value of 0.33 L/h for a healthy neonate of similar age and weight. By introducing TH as a binary covariate on clearance, the additional impact of TH on mannitol clearance was quantified (60% decrease).
Conclusions: Mannitol clearance was decreased by approximately 60% in neonates undergoing TH, although this is likely confounded with asphyxia severity.
Trial registration: ClinicalTrials.gov identifier NCT03162653.
Conflict of interest statement
Neel Deferm, Kim V. Annink, Ruben Faelens, Michael Schroth, Christian A. Maiwald, Loubna el Bakkali, Frank van Bel, Manon J.N.L. Benders, Mirjam M. van Weissenbruch, Anja Hagen, Anne Smits, Pieter Annaert, Axel R. Franz, and Karel Allegaert have no conflicts of interest that are directly relevant to the content of this article. Yannique Jacobs is a collaborator within the ALBINO project and is an employee of ACE Pharmaceuticals, Zeewolde, the Netherlands, which holds the Dutch marketing authorization registration for Acepurin® (allopurinol 1 g/100 mL) for intravenous application for the treatment of gout.
Figures
References
-
- Allegaert K, Smits A, van Donge T, van den Anker J, Sarafidis K, Levtchenko E, et al. Renal precision medicine in neonates and acute kidney injury: how to convert a cloud of creatinine observations to support clinical decisions. Front Pediatr. 2020;8:366. doi: 10.3389/fped.2020.00366. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
