

The role of G-CSF neuroprotective effects in neonatal hypoxic-ischemic encephalopathy (HIE): current status
- PMID: 33612099
- PMCID: PMC7897393
- DOI: 10.1186/s12974-021-02084-4
The role of G-CSF neuroprotective effects in neonatal hypoxic-ischemic encephalopathy (HIE): current status
Abstract
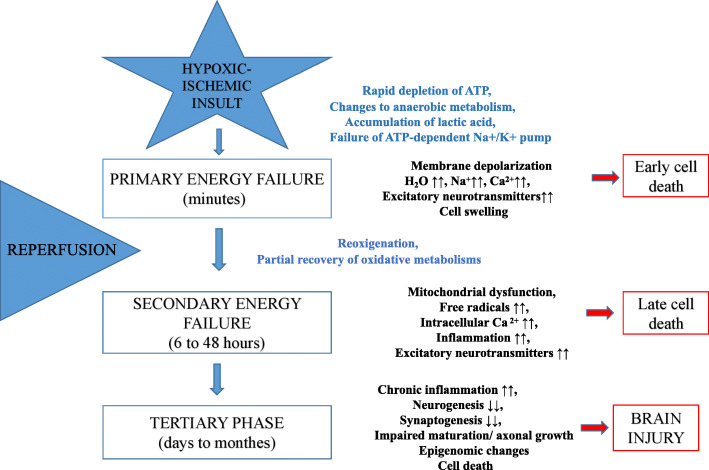
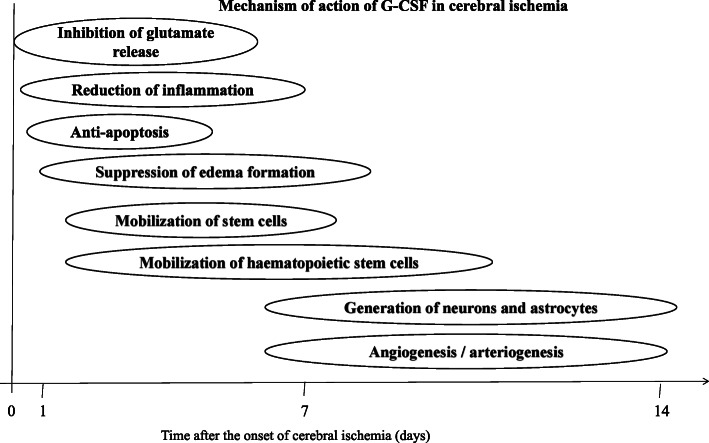
Hypoxic-ischemic encephalopathy (HIE) is an important cause of permanent damage to central nervous system (CNS) that may result in neonatal death or manifest later as mental retardation, epilepsy, cerebral palsy, or developmental delay. The primary cause of this condition is systemic hypoxemia and/or reduced cerebral blood flow with long-lasting neurological disabilities and neurodevelopmental impairment in neonates. About 20 to 25% of infants with HIE die in the neonatal period, and 25-30% of survivors are left with permanent neurodevelopmental abnormalities. The mechanisms of hypoxia-ischemia (HI) include activation and/or stimulation of myriad of cascades such as increased excitotoxicity, oxidative stress, N-methyl-D-aspartic acid (NMDA) receptor hyperexcitability, mitochondrial collapse, inflammation, cell swelling, impaired maturation, and loss of trophic support. Different therapeutic modalities have been implicated in managing neonatal HIE, though translation of most of these regimens into clinical practices is still limited. Therapeutic hypothermia, for instance, is the most widely used standard treatment in neonates with HIE as studies have shown that it can inhibit many steps in the excito-oxidative cascade including secondary energy failure, increases in brain lactic acid, glutamate, and nitric oxide concentration. Granulocyte-colony stimulating factor (G-CSF) is a glycoprotein that has been implicated in stimulation of cell survival, proliferation, and function of neutrophil precursors and mature neutrophils. Extensive studies both in vivo and ex vivo have shown the neuroprotective effect of G-CSF in neurodegenerative diseases and neonatal brain damage via inhibition of apoptosis and inflammation. Yet, there are still few experimentation models of neonatal HIE and G-CSF's effectiveness, and extrapolation of adult stroke models is challenging because of the evolving brain. Here, we review current studies and/or researches of G-CSF's crucial role in regulating these cytokines and apoptotic mediators triggered following neonatal brain injury, as well as driving neurogenesis and angiogenesis post-HI insults.
Keywords: Angiogenesis; Apoptosis; Granulocyte-colony stimulating factor; Hypoxia ischemia; Hypoxic-ischemic encephalopathy; Neonatal; Neurogenesis; Pro-inflammatory cytokine.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
