

First two-stage robotic ALPPS in HCC patients with hepatic vein invasion: a step-by-step procedure from a clinical case
- PMID: 33612103
- PMCID: PMC7898755
- DOI: 10.1186/s12957-021-02170-0
First two-stage robotic ALPPS in HCC patients with hepatic vein invasion: a step-by-step procedure from a clinical case
Abstract
Background: The associating liver partitioning and portal vein occlusion for staged hepatectomy (ALPPS) procedure is gaining interest because it brings hope to patients who cannot undergo radical surgical resection due to insufficient remnant liver volume. However, the indications and technical aspects of this procedure are still under debate. This report demonstrates the technical aspects of the first two-stage robotic ALPPS for HCC.
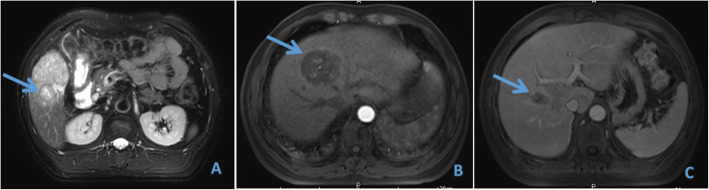
Case presentation: A 55-year-old man with type II portal vein variation was diagnosed with hepatocellular carcinoma. Preoperative 3D reconstruction of the liver based on CT showed a future liver remnant/standard liver volume (FLR/SLV) of 24.45%. The ALPPS procedure was performed using the da Vinci Si system. At the first stage of the operation, we removed the gallbladder and ligated the right anterior branch of the portal vein and the right posterior branch. Following blocking of the hepatic hilum, the liver parenchyma was removed 1 cm away from the right side of the falciform ligament in an incision manner from the top to the bottom and from shallow to deep. The second-stage operation was performed on the 12th postoperative day with a FLR/SLV of 45.13%. During this step, the right hemiliver plus left medial section was separated and removed. Postoperative pathology showed a negative margin. The operative times were 195 and 217 min, respectively. Estimated blood loss was 250 and 500 ml, respectively. There was no need for transfusion or hospitalization in intensive care. The patient was discharged on the 6th postoperative day. Recovery was uneventful after both stages, and the patient did not present any sign of liver failure. Elevation of liver enzymes was minimal. The patient had no evidence of the disease 14 months after the procedure.
Conclusions: The two-stage robotic ALPPS procedure is a safe and feasible technique for select patients with HCC.
Keywords: Associating liver partition and portal vein ligation for staged hepatectomy; Future liver remnant; Hepatocellular carcinoma; Portal vein anomaly; Robotic.
Conflict of interest statement
The authors declare no competing interests.
Figures





Similar articles
-
Impact of split completeness on future liver remnant hypertrophy in associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) in hepatocellular carcinoma: Complete-ALPPS versus partial-ALPPS.Surgery. 2017 Feb;161(2):357-364. doi: 10.1016/j.surg.2016.07.029. Epub 2016 Sep 3. Surgery. 2017. PMID: 27596751
-
Full robotic ALPPS for HCC with intrahepatic portal vein thrombosis.Int J Med Robot. 2020 Apr;16(2):e2087. doi: 10.1002/rcs.2087. Epub 2020 Feb 18. Int J Med Robot. 2020. PMID: 32011081
-
Associating liver partition with portal vein ligation and staged hepatectomy (ALPPS) for the treatment of liver tumors in children.J Pediatr Surg. 2015 Jul;50(7):1227-31. doi: 10.1016/j.jpedsurg.2014.10.019. J Pediatr Surg. 2015. PMID: 25783345
-
Chance and challenge of associating liver partition and portal vein ligation for staged hepatectomy.Hepatobiliary Pancreat Dis Int. 2019 Jun;18(3):214-222. doi: 10.1016/j.hbpd.2019.04.006. Epub 2019 Apr 24. Hepatobiliary Pancreat Dis Int. 2019. PMID: 31056484 Review.
-
Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS): a new strategy to increase resectability in liver surgery.Int J Surg. 2014;12(5):437-41. doi: 10.1016/j.ijsu.2014.03.009. Epub 2014 Apr 2. Int J Surg. 2014. PMID: 24704086 Review.
Cited by
-
Short- and long-term outcomes after robotic and open liver resection for elderly patients with hepatocellular carcinoma: a propensity score-matched study.Surg Endosc. 2022 Nov;36(11):8132-8143. doi: 10.1007/s00464-022-09236-4. Epub 2022 May 9. Surg Endosc. 2022. PMID: 35534731
-
Robotic Complete ALPPS (rALPPS)-First German Experiences.Cancers (Basel). 2024 Mar 6;16(5):1070. doi: 10.3390/cancers16051070. Cancers (Basel). 2024. PMID: 38473426 Free PMC article.
-
Short-term and long-term outcomes after robotic versus open hepatectomy in patients with large hepatocellular carcinoma: a multicenter study.Int J Surg. 2024 Feb 1;110(2):660-667. doi: 10.1097/JS9.0000000000000873. Int J Surg. 2024. PMID: 37983785 Free PMC article.
-
International experts consensus guidelines on robotic liver resection in 2023.World J Gastroenterol. 2023 Aug 28;29(32):4815-4830. doi: 10.3748/wjg.v29.i32.4815. World J Gastroenterol. 2023. PMID: 37701136 Free PMC article. Review.
-
Perioperative impact of liver cirrhosis on robotic liver resection for hepatocellular carcinoma: a retrospective cohort study.Surg Endosc. 2024 Sep;38(9):4926-4938. doi: 10.1007/s00464-024-11032-1. Epub 2024 Jul 8. Surg Endosc. 2024. PMID: 38977502
References
-
- Lang H, de Santibañes E, Schlitt HJ, et al. 10th Anniversary of ALPPS—lessons learned and quo vadis. Ann Surg. 2019;269(1):114–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
