

Indirect acute effects of the COVID-19 pandemic on physical and mental health in the UK: a population-based study
- PMID: 33612430
- PMCID: PMC7985613
- DOI: 10.1016/S2589-7500(21)00017-0
Indirect acute effects of the COVID-19 pandemic on physical and mental health in the UK: a population-based study
Abstract
Background: There are concerns that the response to the COVID-19 pandemic in the UK might have worsened physical and mental health, and reduced use of health services. However, the scale of the problem is unquantified, impeding development of effective mitigations. We aimed to ascertain what has happened to general practice contacts for acute physical and mental health outcomes during the pandemic.
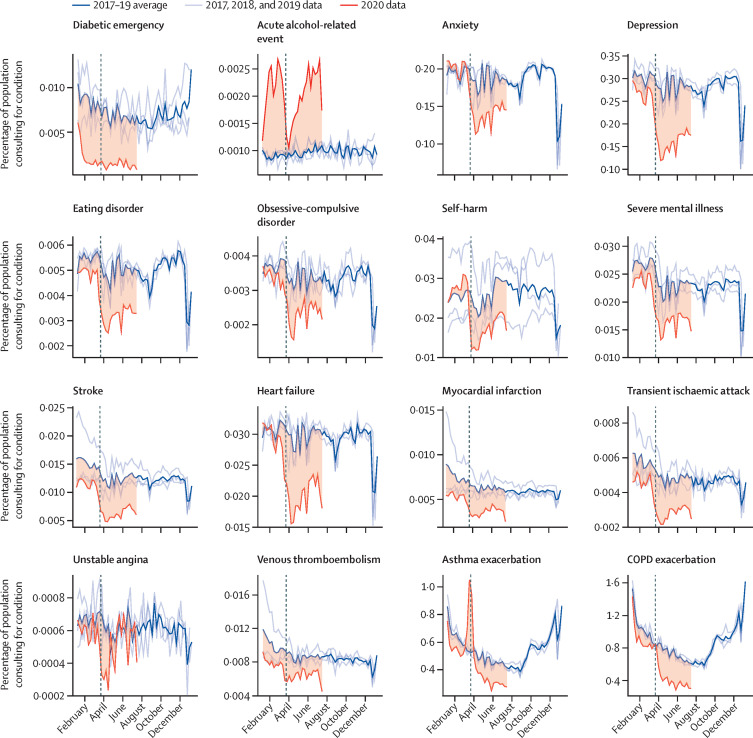
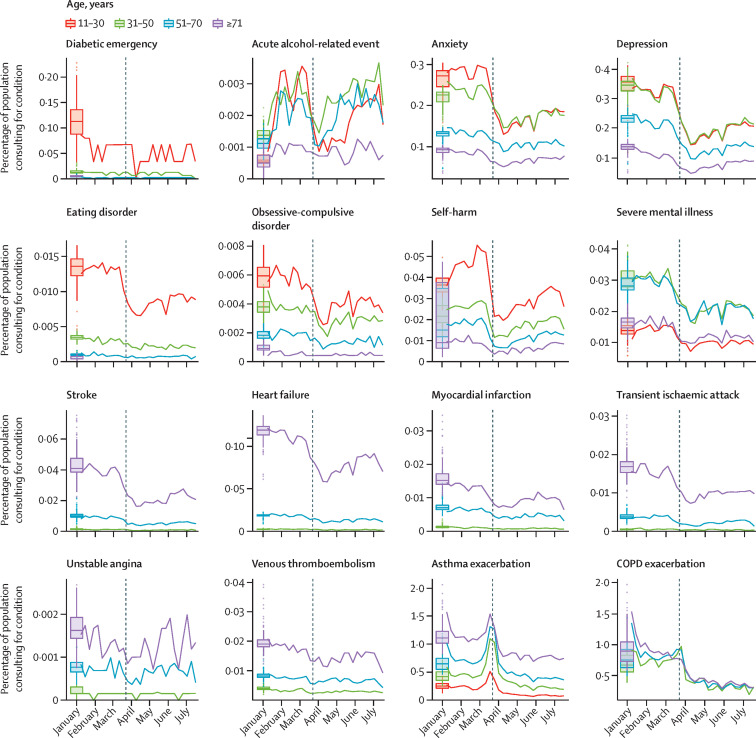
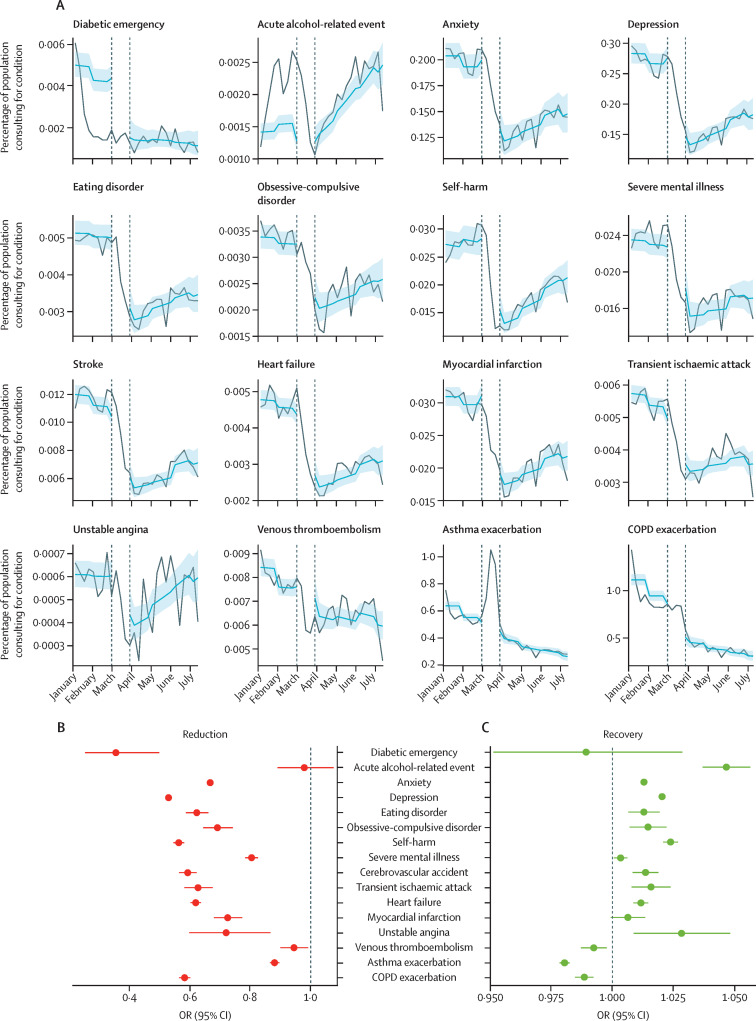
Methods: Using de-identified electronic health records from the Clinical Research Practice Datalink (CPRD) Aurum (covering 13% of the UK population), between 2017 and 2020, we calculated weekly primary care contacts for selected acute physical and mental health conditions: anxiety, depression, self-harm (fatal and non-fatal), severe mental illness, eating disorder, obsessive-compulsive disorder, acute alcohol-related events, asthma exacerbation, chronic obstructive pulmonary disease exacerbation, acute cardiovascular events (cerebrovascular accident, heart failure, myocardial infarction, transient ischaemic attacks, unstable angina, and venous thromboembolism), and diabetic emergency. Primary care contacts included remote and face-to-face consultations, diagnoses from hospital discharge letters, and secondary care referrals, and conditions were identified through primary care records for diagnoses, symptoms, and prescribing. Our overall study population included individuals aged 11 years or older who had at least 1 year of registration with practices contributing to CPRD Aurum in the specified period, but denominator populations varied depending on the condition being analysed. We used an interrupted time-series analysis to formally quantify changes in conditions after the introduction of population-wide restrictions (defined as March 29, 2020) compared with the period before their introduction (defined as Jan 1, 2017 to March 7, 2020), with data excluded for an adjustment-to-restrictions period (March 8-28).
Findings: The overall population included 9 863 903 individuals on Jan 1, 2017, and increased to 10 226 939 by Jan 1, 2020. Primary care contacts for almost all conditions dropped considerably after the introduction of population-wide restrictions. The largest reductions were observed for contacts for diabetic emergencies (odds ratio 0·35 [95% CI 0·25-0·50]), depression (0·53 [0·52-0·53]), and self-harm (0·56 [0·54-0·58]). In the interrupted time-series analysis, with the exception of acute alcohol-related events (0·98 [0·89-1·10]), there was evidence of a reduction in contacts for all conditions (anxiety 0·67 [0·66-0·67], eating disorders 0·62 [0·59-0·66], obsessive-compulsive disorder [0·69 [0·64-0·74]], self-harm 0·56 [0·54-0·58], severe mental illness 0·80 [0·78-0·83], stroke 0·59 [0·56-0·62], transient ischaemic attack 0·63 [0·58-0·67], heart failure 0·62 [0·60-0·64], myocardial infarction 0·72 [0·68-0·77], unstable angina 0·72 [0·60-0·87], venous thromboembolism 0·94 [0·90-0·99], and asthma exacerbation 0·88 [0·86-0·90]). By July, 2020, except for unstable angina and acute alcohol-related events, contacts for all conditions had not recovered to pre-lockdown levels.
Interpretation: There were substantial reductions in primary care contacts for acute physical and mental conditions following the introduction of restrictions, with limited recovery by July, 2020. Further research is needed to ascertain whether these reductions reflect changes in disease frequency or missed opportunities for care. Maintaining health-care access should be a key priority in future public health planning, including further restrictions. The conditions we studied are sufficiently severe that any unmet need will have substantial ramifications for the people with the conditions as well as health-care provision.
Funding: Wellcome Trust Senior Fellowship, Health Data Research UK.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Beyond the tip of the iceberg: direct and indirect effects of COVID-19.Lancet Digit Health. 2021 Apr;3(4):e205-e206. doi: 10.1016/S2589-7500(21)00024-8. Epub 2021 Feb 18. Lancet Digit Health. 2021. PMID: 33612431 Free PMC article. No abstract available.
References
-
- Johns Hopkins University of Medicine COVID-19 dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU) https://coronavirus.jhu.edu/map.html
-
- McConkey R, Wyatt S. The Health Foundation; June 30, 2020. Exploring the fall in A&E visits during the pandemic.https://www.health.org.uk/news-and-comment/charts-and-infographics/explo...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
