

Clinical Presentation and Disease Course of 37 Consecutive Cases of Progressive Multifocal Leukoencephalopathy (PML) at a German Tertiary-Care Hospital: A Retrospective Observational Study
- PMID: 33613439
- PMCID: PMC7890249
- DOI: 10.3389/fneur.2021.632535
Clinical Presentation and Disease Course of 37 Consecutive Cases of Progressive Multifocal Leukoencephalopathy (PML) at a German Tertiary-Care Hospital: A Retrospective Observational Study
Abstract
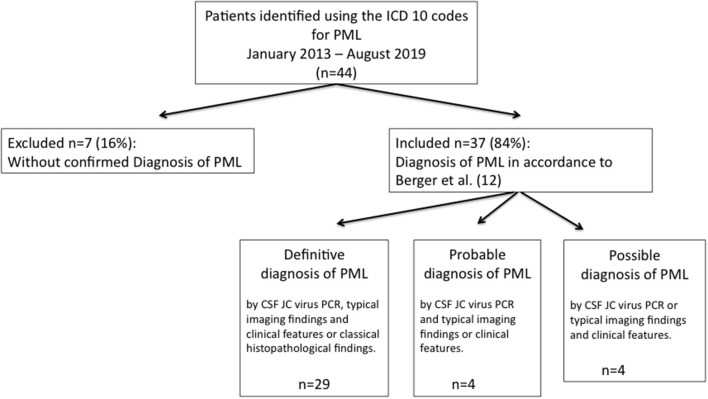
Background: Progressive multifocal leukoencephalopathy (PML) caused by JCV is a rare but frequently fatal disease of the central nervous system, usually affecting immunocompromised individuals. Our study aims to expand the data on patient characteristics, diagnosis, clinical course, possible PML-directed treatment, and outcome of patients with PML at a German tertiary-care hospital. Methods:In this single-center observational cohort study, 37 consecutive patients with a confirmed diagnosis of PML seen at the University Medical Center Hamburg-Eppendorf from 2013 until 2019 were retrospectively analyzed by chart review with a special focus on demographics, risk factors, and clinical aspects as well as PML-directed treatment and survival. Results:We identified 37 patients with definite, probable, and possible PML diagnosis. 36 patients (97%) had underlying immunosuppressive disorders such as HIV/AIDS (n = 17; 46%), previous treatment with monoclonal antibodies (n = 6; 16%), hematological or oncological malignancies (n = 6; 16%), sarcoidosis (n = 5; 14%), solid organ transplantation (n = 1; 3%), and diagnosis of mixed connective tissue disease (n = 1; 3%). In only one patient no evident immunocompromised condition was detected (n = 1; 3%). Treatment attempts to improve the outcome of PML were reported in 13 patients (n = 13; 35%). Twenty seven percent of patients were lost to follow-up (n = 10). Twenty four-month survival rate after diagnosis of PML was 56% (n = 15). Conclusion: This interdisciplinary retrospective study describes epidemiology, risk factors, clinical course, and treatment trials in patients with PML at a German tertiary-care hospital. Acquired immunosuppression due to HIV-1 constituted the leading cause of PML in this monocenter cohort.
Keywords: HIV; JCV; PML-directed treatment; progressive multifocal leukoencephalopathy (PML); risk factors; survival rate.
Copyright © 2021 Graf, Rosenkranz, Hölzemer, Hagel, Goebell, Jordan, Friese, Addo, Schulze zur Wiesch and Beisel.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Clinical Profile and Outcome of Progressive Multifocal Leukoencephalopathy in HIV Infected Indian Patients.J Assoc Physicians India. 2017 Mar;65(3):40-44. J Assoc Physicians India. 2017. PMID: 28462542
-
Progressive multifocal leukoencephalopathy without overt immunosuppression.Medicine (Baltimore). 2023 Sep 29;102(39):e35265. doi: 10.1097/MD.0000000000035265. Medicine (Baltimore). 2023. PMID: 37773871 Free PMC article.
-
Probable progressive multifocal leukoencephalopathy-immune reconstitution inflammatory syndrome with immunosuppressant dose reduction following lung transplantation: a case report and literature review.BMC Neurol. 2019 Oct 31;19(1):263. doi: 10.1186/s12883-019-1493-1. BMC Neurol. 2019. PMID: 31672142 Free PMC article. Review.
-
JC virus DNA load in patients with and without progressive multifocal leukoencephalopathy.Neurology. 1999 Jan 15;52(2):253-60. doi: 10.1212/wnl.52.2.253. Neurology. 1999. PMID: 9932940
-
[Progressive multifocal leukoencephalopathy].Ugeskr Laeger. 1995 Jan 16;157(3):284-8. Ugeskr Laeger. 1995. PMID: 7846775 Review. Danish.
Cited by
-
Virulence of Burkholderia pseudomallei ATS2021 Unintentionally Imported to United States in Aromatherapy Spray.Emerg Infect Dis. 2024 Oct;30(10):2056-2069. doi: 10.3201/eid3010.240084. Emerg Infect Dis. 2024. PMID: 39320153 Free PMC article.
-
Flaccid Brachial Monoplegia As Initial Presentation in a Patient With Progressive Multifocal Leukoencephalopathy.Cureus. 2022 Apr 17;14(4):e24211. doi: 10.7759/cureus.24211. eCollection 2022 Apr. Cureus. 2022. PMID: 35602837 Free PMC article.
-
Nationwide Laboratory Surveillance of Progressive Multifocal Leukoencephalopathy in Japan: Fiscal Years 2011-2020.Viruses. 2023 Apr 14;15(4):968. doi: 10.3390/v15040968. Viruses. 2023. PMID: 37112948 Free PMC article.
-
An Elusive Target: Inhibitors of JC Polyomavirus Infection and Their Development as Therapeutics for the Treatment of Progressive Multifocal Leukoencephalopathy.Int J Mol Sci. 2023 May 11;24(10):8580. doi: 10.3390/ijms24108580. Int J Mol Sci. 2023. PMID: 37239927 Free PMC article. Review.
-
Progressive multifocal leukoencephalopathy and spectrum of predisposing conditions: a 20-year retrospective cohort study in a tertiary center in São Paulo, Brazil.Neurol Sci. 2025 Jan;46(1):365-379. doi: 10.1007/s10072-024-07669-4. Epub 2024 Jul 15. Neurol Sci. 2025. PMID: 39007964
References
LinkOut - more resources
Full Text Sources
Other Literature Sources