

Autoantibodies Against Lysosome Associated Membrane Protein-2 (LAMP-2) in Pediatric Chronic Primary Systemic Vasculitis
- PMID: 33613565
- PMCID: PMC7893977
- DOI: 10.3389/fimmu.2020.624758
Autoantibodies Against Lysosome Associated Membrane Protein-2 (LAMP-2) in Pediatric Chronic Primary Systemic Vasculitis
Abstract
Background: Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) is a small vessel vasculitis in adults and children that commonly affects the kidneys. Although the frequent antigenic, and presumed pathogenic, targets of ANCA in AAV are proteinase-3 (PR3) and myeloperoxidase (MPO), ANCA against lysosome associated membrane protein-2 (LAMP-2), a lesser known ANCA antigen that is expressed on the glomerular endothelium, are present in some adults with AAV-associated renal disease. LAMP-2-ANCA has not been assessed in children with chronic systemic vasculitis, and, if present, would be a potentially valuable biomarker given that treatment decisions for these pediatric patients at diagnosis are largely informed by kidney function.
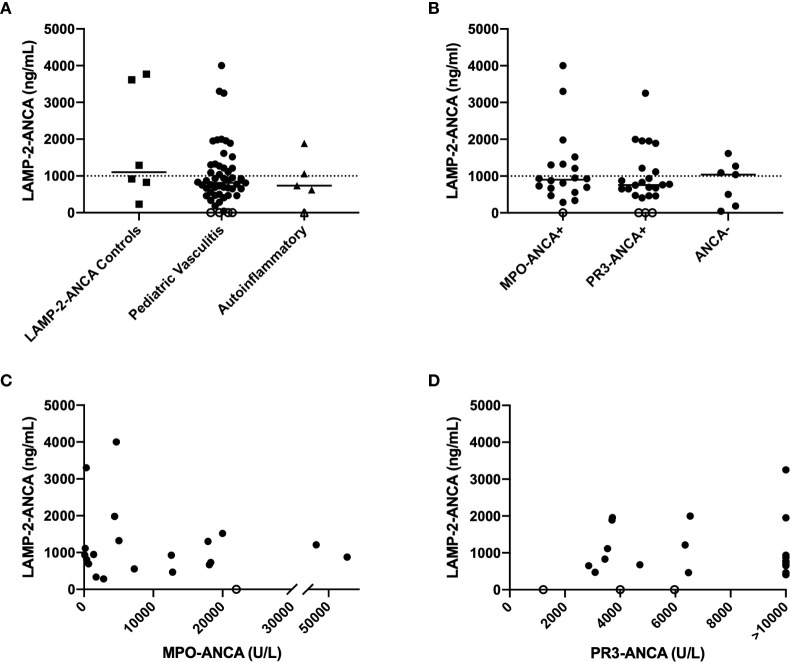
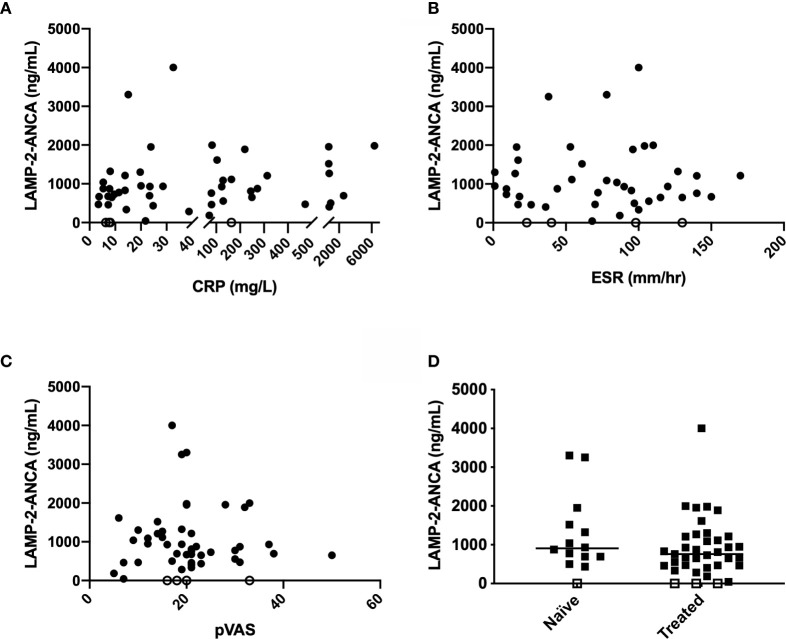
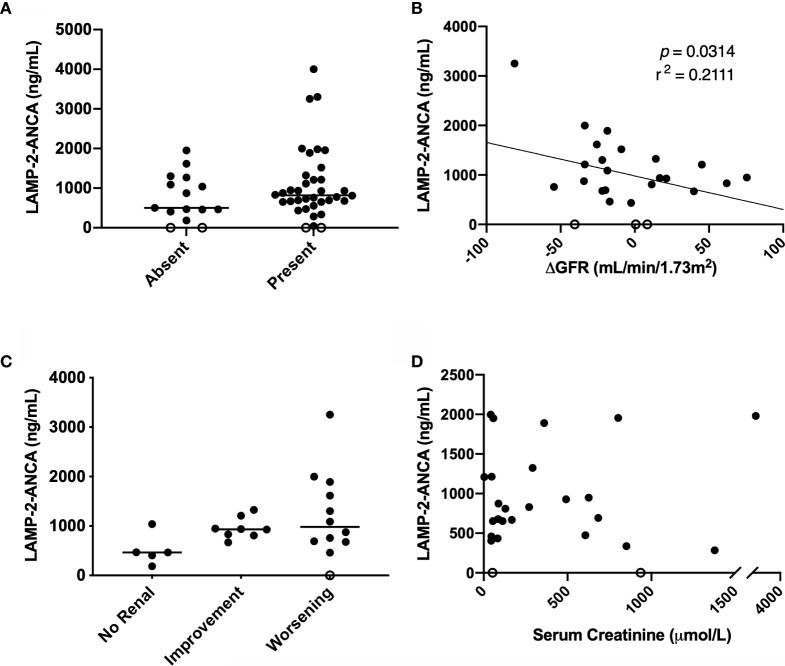
Methods: A custom ELISA, using commercially available reagents, was designed to detect autoantibodies to human LAMP-2 in serum. Sera obtained from 51 pediatric patients at the time of diagnosis of chronic primary systemic vasculitis (predominantly AAV) were screened. LAMP-2-ANCA titers were evaluated for correlation with clinical metrics of disease activity (pediatric vasculitis activity score [pVAS], C-reactive protein [CRP] concentration, and erythrocyte sedimentation rate [ESR]), MPO- and PR3-ANCA titers, and renal function (glomerular filtration rate [GFR], renal-specific pVAS, and serum creatinine concentration).
Results: LAMP-2-ANCA (>1,000 ng/ml) were detected in 35% (n = 18) of pediatric systemic vasculitis patients, of which, 10 (20% of all patients) were found to have high positive titers (>1,500 ng/ml). Undetectable or negative titres (<500 ng/ml) were identified in 12% (n = 6) of patients, those with titers between 500 and 1,000 ng/ml were considered low with unknown clinical relevance (53%, n = 27). Although LAMP-2-ANCA titers did not significantly differ between patients with AAV versus ANCA-negative vasculitis, only AAV patients had high concentrations (>1,500 ng/ml) of LAMP-2-ANCA. LAMP-2-ANCA titers did not correlate with measures of disease activity (pVAS, CRP, or ESR) at the time of diagnosis. In contrast, for patients with 12-month post diagnosis follow-up, a negative correlation was observed between the change in GFR (from diagnosis to 12-month follow-up) and LAMP-2-ANCA titer at diagnosis.
Conclusions: Moderate to high LAMP-2-ANCA titers were detected in 35% (18/51) of children with chronic systemic vasculitis affecting small-to-medium vessels. Although the highest concentrations of LAMP-2-ANCA in this population were observed in individuals positive for classic ANCA (MPO- or PR3-ANCA), similar to previous reports on adult patients, LAMP-2-ANCA titers do not correlate with classic ANCA titers or with overall disease activity at diagnosis. Renal disease is a common manifestation in systemic small-medium vessel vasculitis (both in adults and children, though more severe in children) and our preliminary data suggest LAMP-2-ANCA at diagnosis may be a risk factor for more severe renal disease.
Keywords: ANCA-associated vasculitis; LAMP-2; anti-neutrophil cytoplasmic antibody; lysosome-associated membrane protein-2; pediatric; systemic vasculitis.
Copyright © 2021 Gibson, Kain, Luqmani, Ross, Cabral and Brown.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Anti-LAMP-2 Antibody Seropositivity in Children with Primary Systemic Vasculitis Affecting Medium- and Large-Sized Vessels.Int J Mol Sci. 2024 Mar 28;25(7):3771. doi: 10.3390/ijms25073771. Int J Mol Sci. 2024. PMID: 38612581 Free PMC article.
-
Clinical characteristics of patients with vasculitis positive for anti-neutrophil cytoplasmic antibody targeting both proteinase 3 and myeloperoxidase: a retrospective study.Rheumatol Int. 2019 Nov;39(11):1919-1926. doi: 10.1007/s00296-019-04447-w. Epub 2019 Sep 24. Rheumatol Int. 2019. PMID: 31552433
-
Assessment of the correlation of commonly used laboratory tests with clinical activity, renal involvement and treatment of systemic small-vessel vasculitis with the presence of ANCA antibodies.BMC Nephrol. 2021 Aug 26;22(1):290. doi: 10.1186/s12882-021-02495-8. BMC Nephrol. 2021. PMID: 34445984 Free PMC article.
-
New advances in the pathogenesis of ANCA-associated vasculitides.Clin Exp Rheumatol. 2009 Jan-Feb;27(1 Suppl 52):S108-14. Clin Exp Rheumatol. 2009. PMID: 19646356 Review.
-
The Diagnostic and Clinical Utility of Autoantibodies in Systemic Vasculitis.Antibodies (Basel). 2019 May 1;8(2):31. doi: 10.3390/antib8020031. Antibodies (Basel). 2019. PMID: 31544837 Free PMC article. Review.
Cited by
-
Kidney immunology from pathophysiology to clinical translation.Nat Rev Immunol. 2025 Jun;25(6):460-476. doi: 10.1038/s41577-025-01131-y. Epub 2025 Jan 30. Nat Rev Immunol. 2025. PMID: 39885266 Review.
-
Childhood-Onset ANCA-Associated Vasculitis: From Genetic Studies to Advances in Pathogenesis, Classification and Novel Therapeutic Approaches.Int J Mol Sci. 2024 Dec 22;25(24):13704. doi: 10.3390/ijms252413704. Int J Mol Sci. 2024. PMID: 39769465 Free PMC article. Review.
-
Knockout of the neonatal Fc receptor alters immune complex trafficking and lysosomal function in cultured podocytes.PLoS One. 2023 Apr 18;18(4):e0284636. doi: 10.1371/journal.pone.0284636. eCollection 2023. PLoS One. 2023. PMID: 37071647 Free PMC article.
-
The correlation between obesity and the occurrence and development of breast cancer.Eur J Med Res. 2025 May 26;30(1):419. doi: 10.1186/s40001-025-02659-4. Eur J Med Res. 2025. PMID: 40414892 Free PMC article. Review.
-
Anti-LAMP-2 Antibody Seropositivity in Children with Primary Systemic Vasculitis Affecting Medium- and Large-Sized Vessels.Int J Mol Sci. 2024 Mar 28;25(7):3771. doi: 10.3390/ijms25073771. Int J Mol Sci. 2024. PMID: 38612581 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous